


What is Diabetic Retinopathy (DR)?
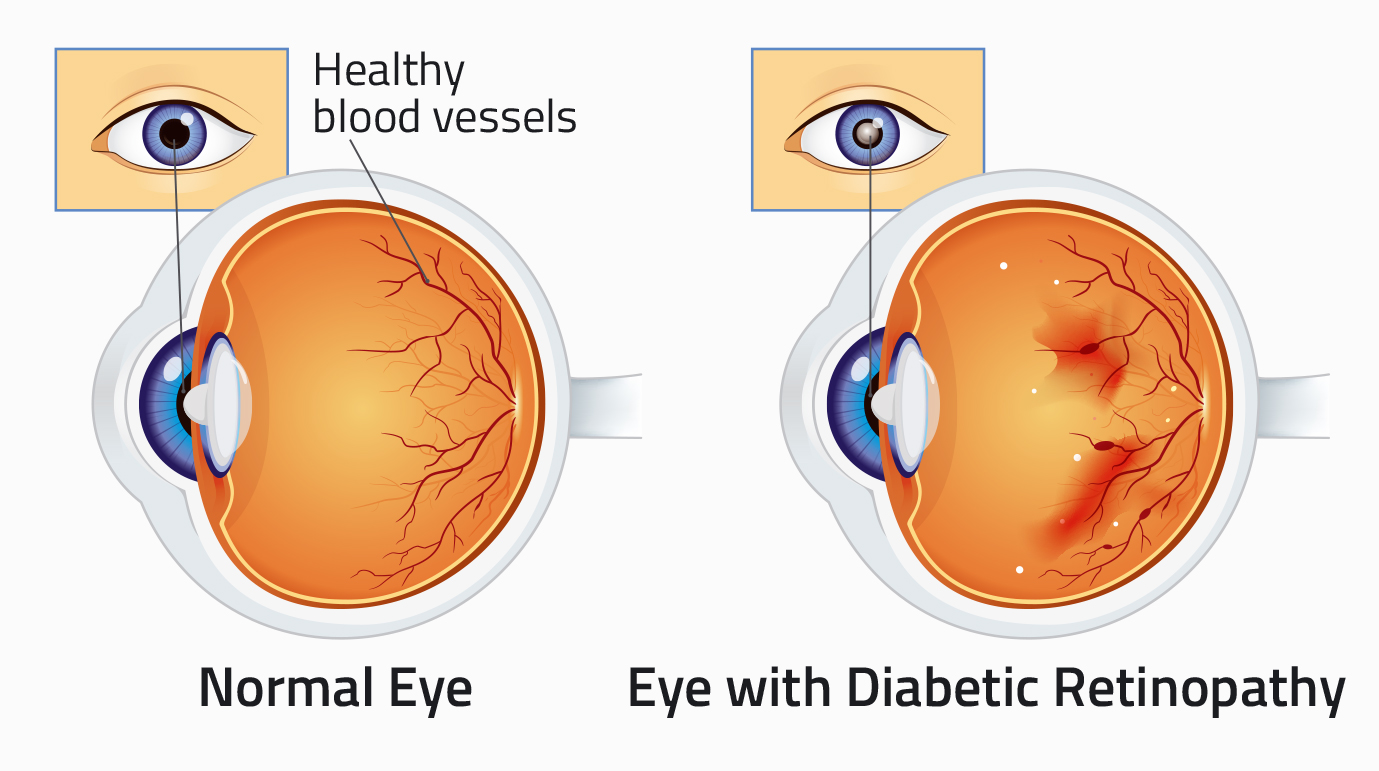
People with diabetes can develop an eye disease called Diabetic Retinopathy. This is when high blood sugar levels damage the blood vessels in the retina.
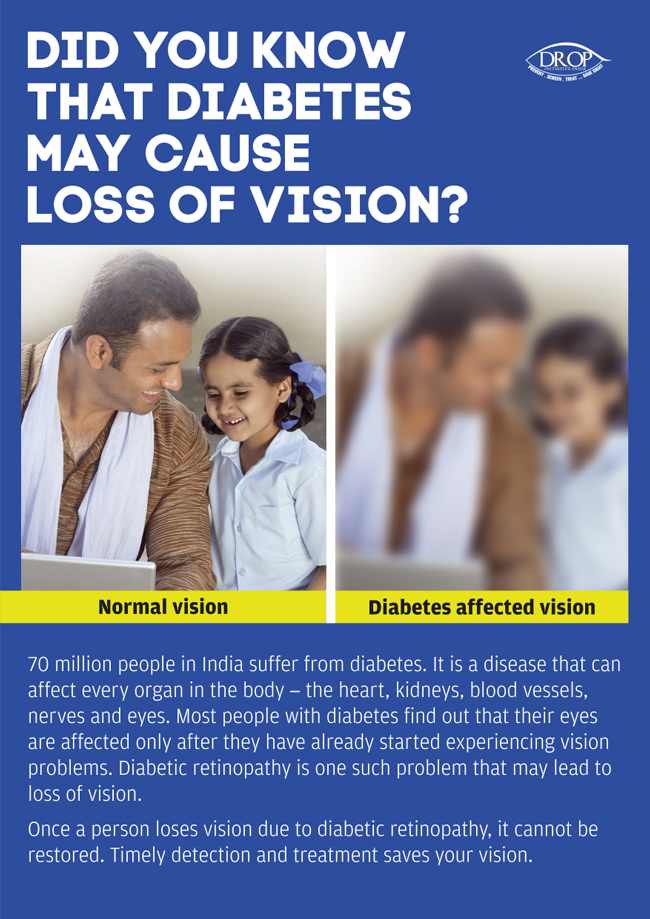
The retina is a light-sensitive part of the inside of the eye. Damage to the retina can lead to loss of vision. As the retina is inside the eye, damage might be occurring but the eyes look entirely normal.
In Diabetic Retinopathy the retinal blood vessels become leaky, or blocked. All of the following can lead to loss of vision:
- Leaky blood vessels can cause swelling of the retina
- Blocked blood vessels cause damage because not enough oxygen reaches the retina
- Abnormal blood vessels can grow on the retina. These blood vessels can cause bleeding inside the eye
Symptoms
In the early stages of Diabetic Retinopathy, the vision is usually not affected. As the retinopathy progresses the vision can be affected. If the condition is ignored for a long time, it can lead to complete loss of sight.
Important
The risk of Diabetic Retinopathy is reduced if blood sugar levels and blood pressure are well controlled.
Should Diabetic Retinopathy develop, if detected early, it can be treated to preserve your vision. Once vision has been lost it cannot usually be restored.
Technical Guidelines
The scope of these Technical Guidelines is wide, and includes recommendations for the following:
- the prevention of Diabetic Retinopathy in people with diabetes
- approaches to the early detection of Diabetic Retinopathy by screening and opportunistic examination
- clinical investigations for the diagnosis of retinopathy
- clinical management of the different types and stages
The Guidelines also include recommendations for the management of cataract in people with diabetes with respect to the prevention and management of Diabetic Retinopathy. It does not include the primary prevention of diabetes, the control of risk factors for other complications of diabetes, nor vision rehabilitation.
The purpose of the Guidelines is to provide recommendations to relevant audiences, anticipating the likely increase in the incidence of visual impairment and blindness from Diabetic Retinopathy as the diabetes ‘epidemic’ in India continues and matures. The Guidelines are intended for a wide audience, including policy makers and service planners and a wide range of health care professionals who provide services for people with diabetes and eye care at all levels in the health system.
Given the wide scope of the Guidelines, many of the recommendations are for practice, in relation to clinical management and for public health. These technical Guidelines are supported by Operational Guidelines which go into more detail about how a programme for the control of visual loss from diabetic retinopathy can be implanted through integration into the health system in India.
DR Grading – Training: Link to CERA Website
Centre for Eye Health Research’s (CERA) online self-directed Diabetic Retinopathy Grading Course for health professionals is for anyone interested in grading retinal changes associated with diabetes, especially those using non mydriatic retinal photography. The course is divided into several topics and contains practice sessions at the end of each topic. At the end there is a competency based exam that is divided into three short assessments; it can be repeated as many times as required.
The exam tests users’ ability to detect and grade retinopathy, as well as determine the appropriate referral timelines for retinopathy. A certificate of competency is awarded on successful completion of the examinations.
Certificate Course in Evidence-Based Management of Diabetic Retinopathy
Certificate course in Evidence-Based Management of Diabetic Retinopathy is a certificate programme to enhance knowledge, skills and core competencies of practicing primary care physicians in management of Diabetic Retinopathy. This course helps to develop a standard teaching protocol and module for evidence based learning on Diabetic Retinopathy. The CCDR course enables primary care physicians to build a network and update them with the latest advancements in the field of Diabetic Retinopathy.
The CCDR course is a joint certificate programme designed, implemented and delivered by Public Health Foundation of India in collaboration with academic partners Dr Mohan’s Diabetes Education Academy (DMDEA) and Aravind Eye Care System. The educational grant for the same has been provided by The Queen Elizabeth Diamond Jubilee Trust (QEDJT) with funding from The Leona M. and Harry B. Helmsley Charitable Trust.
Publication Links

Link to special issue IJEM
The Diabetic Retinopathy special issue of Indian Journal of Endocrinology and Metabolism documents the current status of diabetes-related eye care infrastructure in India. It is a valuable resource for physicians, diabetologists, and endocrinologists. In addition to the estimates of the burden of disease in the country, the document also suggests the need for an increased national focus on this cause of avoidable blindness.

Community Eye Health Journal on DR
The diabetic eye diseases special issue of the Community Eye Health Journal discusses various aspects of management and treatment of Diabetic Retinopathy. It also has several art clinical and technical articles to update and inform your diagnosis and management of DR patients.
Operational Guidelines
In India diabetes mellitus is fast gaining the status of an epidemic, with 62 million people diagnosed with the disease and this number is likely to go up to 79.4 million by 2030 as per WHO reports.
Diabetic Retinopathy (DR) is one of the complications of diabetes mellitus (incidence ranging from 6-30%),and is a leading cause of visual impairment and avoidable blindness. The manifestations of DR may vary from mild background retinopathy to severe sight threatening proliferative retinopathy/macular edema. The early stages of DR, which are symptomless, are treatable, if detected and managed in time. The sad fact is that by the time the diabetic patient reaches the ophthalmologist, DR is already in an advanced stage, and the visual prognosis is bleak. This is due to lack of awareness and sensitisation not only among patients but also among medical professionals and the treating physicians/endocrinologists.
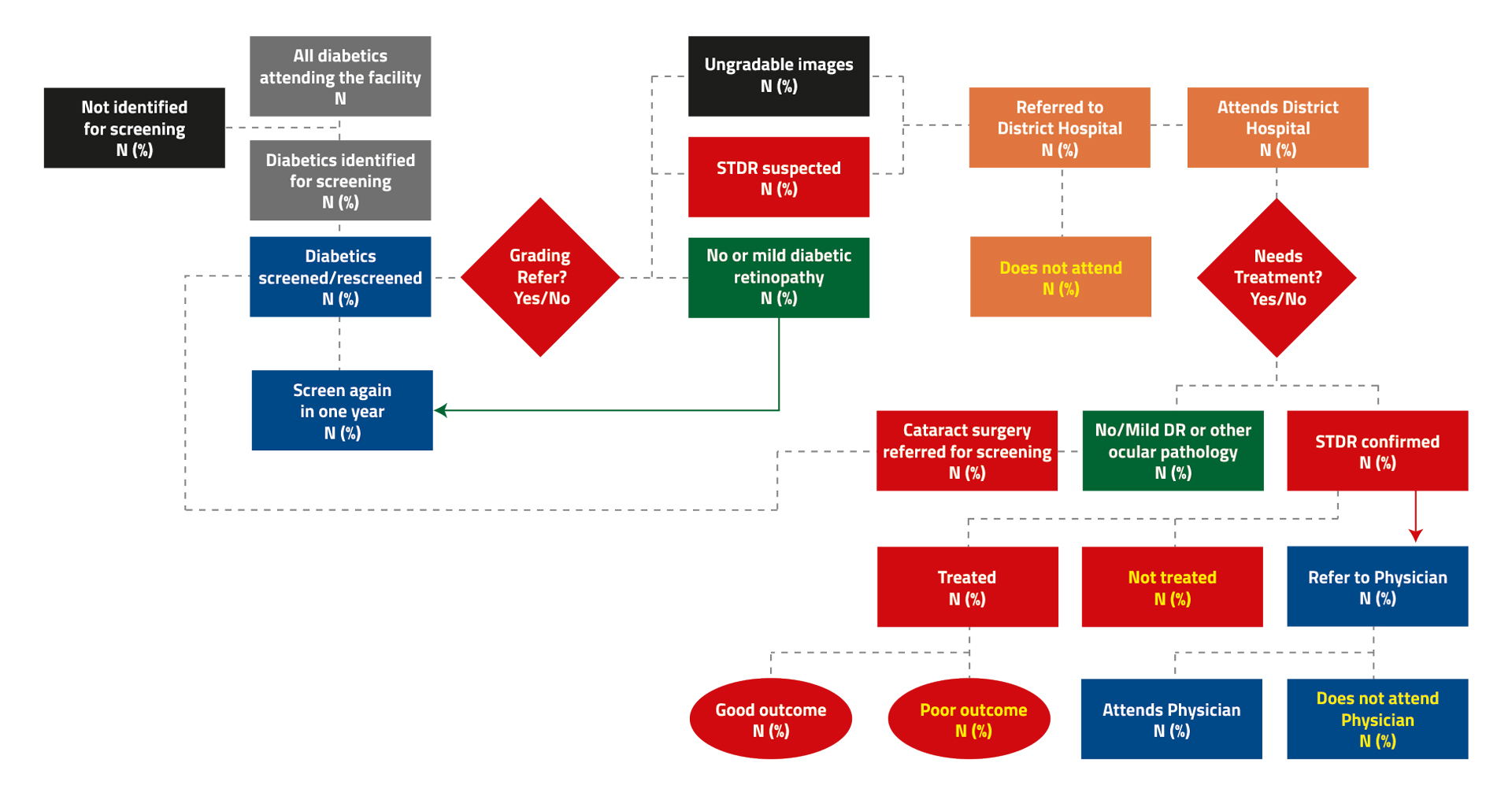
These operational guidelines for management of Diabetic Retinopathy have thus come at a very opportune moment. They provide a broad framework for the policy makers and planners for integration between two National Health Programmes viz, the NPCDCS (National Programme for Cancer, Diabetes, Cardiac diseases and Stroke) and NPCBVI(National Programme for Control of Blindness & Visual Impairment) through opportunistic screening of diabetic patients attending NCD clinics which have been set up in all district and sub district Hospitals. The use of teleophthalmology as an important tool (to be used by specially trained PMOAs/ Nurses) at health & wellness centers for opportunistic screening of diabetics attending the NCD clinics and sending the doubtful images to the Ophthalmologists for confirmation of DR Grading has been well conceptualised. This would help in minimising the drop outs among diabetics and a better utilization of the already crunched manpower of ophthalmologists. The guidelines also illustrate the set of interventions required at various levels of health care that need to be taken for prevention, early detection and treatment of DR cases.
These guidelines will benefit the patients, medical experts and ophthalmologists and go a long way in reducing the burden of avoidable blindness due to DR in our Country.

Standard Operating Procedure for Ophthalmic Officers for DR screening
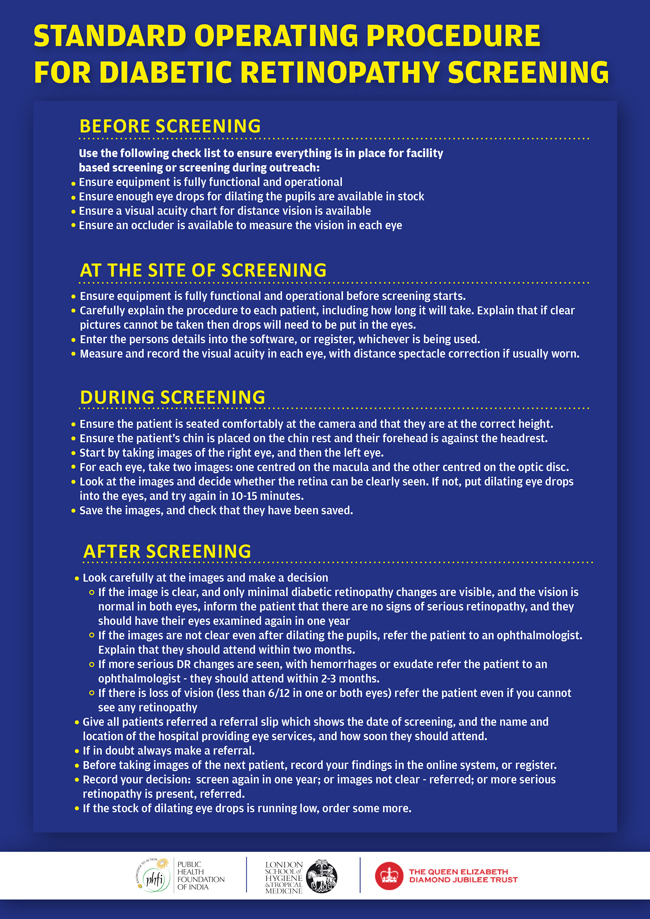
Use the following check list to ensure everything is in place for facility based screening or screening during outreach:
- Ensure equipment is fully functional and operational
- Ensure enough eye drops for dilating the pupils are available in stock
- Ensure a visual acuity chart for distance vision is available
- Ensure an occluder is available to measure the vision in each eye
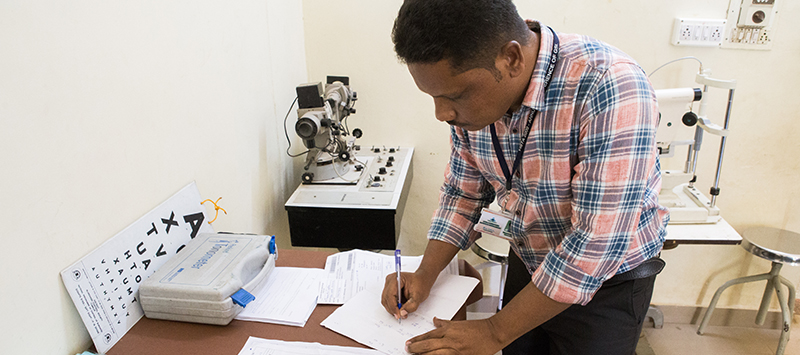
An ophthalmic officer using a checklist for DR screening at Tumkur, India
- Ensure equipment is fully functional and operational before screening starts
- Carefully explain the procedure to each patient, including how long it will take. Explain that if clear pictures cannot be taken then drops will need to be put in the eyes
- Enter the person’s details into the software, or register, whichever is being used
- Measure and record the visual acuity in each eye, with distance spectacle correction if usually worn

- Ensure the patient is seated comfortably at the camera and that they are at the correct height
- Ensure the patient’s chin is placed on the chin rest and their forehead is against the headrest
- Start by taking images of the right eye, and then the left eye
- For each eye, take two images: one centred on the macula and the other centred on the optic disc
- Look at the images and decide whether the retina can be clearly seen. If not, put dilating eye drops into the eyes, and try again in 10-15 minutes
- Save the images, and check that they have been saved

Look carefully at the images and make a decision:
- If the image is clear, and only minimal Diabetic Retinopathy changes are visible, and the vision is normal in both eyes, inform the patient that there are no signs of serious Retinopathy, and they should have their eyes examined again in one year
- If the images are not clear even after dilating the pupils, refer the patient to an ophthalmologist. Explain that they should attend within two months.
- If more serious DR changes are seen, with hemorrhages or exudate, refer the patient to an ophthalmologist – they should attend within two to three months.
- If there is loss of vision (less than 6/12 in one or both eyes) refer the patient even if you cannot see any Retinopathy
Give all referred patients a referral slip which shows the date of screening, and the name and location of the hospital providing eye services, and how soon they should attend:
- If in doubt always make a referral
- Before taking images of the next patient, record your findings in the online system, or register
- Record your decision: screen again in one year; or images not clear – referred; or more serious Retinopathy is present, referred
- If the stock of dilating eye drops is running low, order some more

- Before Screening
Use the following check list to ensure everything is in place for facility based screening or screening during outreach:
- Ensure equipment is fully functional and operational
- Ensure enough eye drops for dilating the pupils are available in stock
- Ensure a visual acuity chart for distance vision is available
- Ensure an occluder is available to measure the vision in each eye
An ophthalmic officer using a checklist for DR screening at Tumkur, India- At the Site of Screening
- Ensure equipment is fully functional and operational before screening starts
- Carefully explain the procedure to each patient, including how long it will take. Explain that if clear pictures cannot be taken then drops will need to be put in the eyes
- Enter the person’s details into the software, or register, whichever is being used
- Measure and record the visual acuity in each eye, with distance spectacle correction if usually worn
- During Screening
- Ensure the patient is seated comfortably at the camera and that they are at the correct height
- Ensure the patient’s chin is placed on the chin rest and their forehead is against the headrest
- Start by taking images of the right eye, and then the left eye
- For each eye, take two images: one centred on the macula and the other centred on the optic disc
- Look at the images and decide whether the retina can be clearly seen. If not, put dilating eye drops into the eyes, and try again in 10-15 minutes
- Save the images, and check that they have been saved
- After Screening
Look carefully at the images and make a decision:
- If the image is clear, and only minimal Diabetic Retinopathy changes are visible, and the vision is normal in both eyes, inform the patient that there are no signs of serious Retinopathy, and they should have their eyes examined again in one year
- If the images are not clear even after dilating the pupils, refer the patient to an ophthalmologist. Explain that they should attend within two months.
- If more serious DR changes are seen, with hemorrhages or exudate, refer the patient to an ophthalmologist – they should attend within two to three months.
- If there is loss of vision (less than 6/12 in one or both eyes) refer the patient even if you cannot see any Retinopathy
Give all referred patients a referral slip which shows the date of screening, and the name and location of the hospital providing eye services, and how soon they should attend:
- If in doubt always make a referral
- Before taking images of the next patient, record your findings in the online system, or register
- Record your decision: screen again in one year; or images not clear – referred; or more serious Retinopathy is present, referred
- If the stock of dilating eye drops is running low, order some more
Useful Links
| State | Training Institution | Website |
|---|---|---|
| Andhra Pradesh | PVRI Hyderabad | |
| Goa | HV Desai Eye Hospital, Pune (Current training institution for Ophthalmologists from Goa) | |
| Gujarat | Divyajyoti Trust, Mandvi, Surat (Dist.) | |
| Karnataka | VIIO Bangalore | |
| Kerala | Little Flower Hospital, Thrissur | |
| Maharashtra | MGIMS, Wardha | |
| Odisha | LV Prasad Eye Institute, Bhubaneshwar | |
| Rajasthan | Global Hospital, Mount Abu | |
| Tamil Nadu | Aravind Eye Hospital, Tirunelveli | |
| West Bengal | VMANN, Rural West Bengal | n/a |
| State | DR Screening Centres under the Project | DR Treatment Centres under the Project |
|---|---|---|
| Andhra Pradesh | CHC - Bobbili | PVRI - Vizainagaram |
| CHC - Cheepurpalli | ||
| Area Hospital - Parvathipuram | ||
| District Hospital - Vizainagaram | ||
| Odisha | CHC - Botalama | Capital Hospital - Bhubaneshwar |
| CHC - Balakati | ||
| CHC - Jatni | ||
| District Hospital - Khurda | ||
| West Bengal | CHC - Sabang | Medinipur Medical College (MMC) |
| CHC - Daspur | ||
| CHC - Garbeta | ||
| CHC - Sonakhali | ||
| CHC - Vidyasagar | ||
| CHC - Keshiyaari | ||
| District Hospital - Kharagpur | ||
| District Hospital - Ghatal | ||
| Gujarat | CHC - Areth | Divyajyoti Hospital, Mandvi (Surat Dist.) |
| CHC - Umarpada | ||
| CHC - Zankhvav | ||
| CHC - Mangrol | ||
| Goa | North Goa District Hospital (Asilio) - Mapusa | Goa Medical College (GMC), Bambolim |
| South Goa District Hospital (Hospicio) - Margao | ||
| Sub-District Hospital - Ponda | ||
| Cottage Hospital - Chicalim | ||
| CHC - Canacona | ||
| PHC - Sankhali | ||
| Maharashtra | Rural hospital - Seloo | MGIMS, Wardha |
| Rural Hospital - Hinganghat | ||
| Sub-District Hospital - Arvi | ||
| Civil Hospital - Wardha | ||
| Kerala | CHC - Chalakuddy | Little Flower Hospital, Thrissur / equipment recently transferred to DH |
| CHC - Chavakkad | ||
| CHC - Kunnamkulum | ||
| Taluk Hospital - Kodungalloor | ||
| Thrissur General Hospital | ||
| Tamilnadu | Upgraded PHC - Thisayanvilai | 1. District Hospital - Tirunelveli 2. Aravind Eye Hospital - Tirunelveli |
| Upgraded PHC - Thirukurunkudi | ||
| Upgraded PHC - Mukkudal | ||
| Upgraded PHC - Ukkirankottai | ||
| Upgraded PHC - Vairavikulum | ||
| District Hospital, Medical College & Hospital - Tirunelveli | ||
| Rajasthan | CHC - Sumerpur | 1. District Hospital - Pali 2. Global Hospital - Mount Abu |
| CHC - Sadri | ||
| CHC - Sojat | ||
| CHC - Jaitaran | ||
| District Hospital - Pali | ||
| Karnataka | CHC - Koratagere | 1. VIIO-operated Mobile Vans 2. At VIIO premises in Bangalore |
| CHC - Gubbi | ||
| CHC - Pavagada | ||
| CHC - Madhugiri | ||
| District Hospital - Tumkur |
- Links to Training Institutions
State Training Institution Website Andhra Pradesh PVRI Hyderabad Goa HV Desai Eye Hospital, Pune (Current training institution for Ophthalmologists from Goa) Gujarat Divyajyoti Trust, Mandvi, Surat (Dist.) Karnataka VIIO Bangalore Kerala Little Flower Hospital, Thrissur Maharashtra MGIMS, Wardha Odisha LV Prasad Eye Institute, Bhubaneshwar Rajasthan Global Hospital, Mount Abu Tamil Nadu Aravind Eye Hospital, Tirunelveli West Bengal VMANN, Rural West Bengal n/a - DR Screening/Treatment Centres under the Project
State DR Screening Centres under the Project DR Treatment Centres under the Project Andhra Pradesh CHC - Bobbili PVRI - Vizainagaram CHC - Cheepurpalli Area Hospital - Parvathipuram District Hospital - Vizainagaram Odisha CHC - Botalama Capital Hospital - Bhubaneshwar CHC - Balakati CHC - Jatni District Hospital - Khurda West Bengal CHC - Sabang Medinipur Medical College (MMC) CHC - Daspur CHC - Garbeta CHC - Sonakhali CHC - Vidyasagar CHC - Keshiyaari District Hospital - Kharagpur District Hospital - Ghatal Gujarat CHC - Areth Divyajyoti Hospital, Mandvi (Surat Dist.) CHC - Umarpada CHC - Zankhvav CHC - Mangrol Goa North Goa District Hospital (Asilio) - Mapusa Goa Medical College (GMC), Bambolim South Goa District Hospital (Hospicio) - Margao Sub-District Hospital - Ponda Cottage Hospital - Chicalim CHC - Canacona PHC - Sankhali Maharashtra Rural hospital - Seloo MGIMS, Wardha Rural Hospital - Hinganghat Sub-District Hospital - Arvi Civil Hospital - Wardha Kerala CHC - Chalakuddy Little Flower Hospital, Thrissur / equipment recently transferred to DH CHC - Chavakkad CHC - Kunnamkulum Taluk Hospital - Kodungalloor Thrissur General Hospital Tamilnadu Upgraded PHC - Thisayanvilai 1. District Hospital - Tirunelveli
2. Aravind Eye Hospital - TirunelveliUpgraded PHC - Thirukurunkudi Upgraded PHC - Mukkudal Upgraded PHC - Ukkirankottai Upgraded PHC - Vairavikulum District Hospital, Medical College & Hospital - Tirunelveli Rajasthan CHC - Sumerpur 1. District Hospital - Pali
2. Global Hospital - Mount AbuCHC - Sadri CHC - Sojat CHC - Jaitaran District Hospital - Pali Karnataka CHC - Koratagere 1. VIIO-operated Mobile Vans
2. At VIIO premises in BangaloreCHC - Gubbi CHC - Pavagada CHC - Madhugiri District Hospital - Tumkur

Case Studies
Deva Devika works as a nurse for non-communicable diseases at community health centre (CHC) in Thisayanvilai. She has been in service since 2012. She has been part of the Diabetic Retinopathy project right from the start. She attended four-day training at Aravind Eye Hospital, Tirunelveli. Deva Devika has helped screen 720 patients for Diabetic Retinopathy and has identified 50 of them who are eligible for treatment.
“I am proud to be a part of this project. Because of this project, many patients in my centre now know about diabetes and how it affects the eyes. This is one of the most useful programmes for the people in rural areas. Through this project, I too have learned about DR and to capture fundus images. Although the treatment for DR is free of cost, the challenge is to make the people to go for regular follow-up and treatment.
This project has made patients with diabetes in my centre aware about DR, and its prevention and treatment. I thank the project, Aravind Eye Hospital and Government of Tamil Nadu for this wonderful initiative.

Dr Venugopal is the head of Retina-Vitreous Services at Aravind Eye Hospital, Tirunelveli. He started his career at Aravind Eye Hospital as a medical officer in 2010 and rose to become a consultant in 2012. He has published papers in 10 international journals so far. His areas of interest are vitreo-retinal diseases and ocular trauma/infections/inflammation/paediatric retina.
Dr Venugopal is part of the DR project and helped to screen and treat many patients for DR. He has trained ophthalmologists and general physicians in fluorescein angiography and optical coherence tomography as part of the Trust DR programme.
“I am glad to contribute my knowledge in capacity building of physicians and ophthalmologists as part of the Trust project. I also wish that there were more LASER treatment options for the Diabetic Retinopathy patients in Tirunelveli district. Such a self-sustainable model would help the government health system to cater for the needy people.
As a member of Aravind Eye Care System, I thank the QEDJT for providing me such a rare opportunity in my career to share my learning with others. Scaling up of this project to all parts of the country can help save many from going blind in India.”

- Case Study: Ms Lakshmi
- Case Study: Dr Dinesh Kumar
- Case Study: A proud NCD Nurse
Deva Devika works as a nurse for non-communicable diseases at community health centre (CHC) in Thisayanvilai. She has been in service since 2012. She has been part of the Diabetic Retinopathy project right from the start. She attended four-day training at Aravind Eye Hospital, Tirunelveli. Deva Devika has helped screen 720 patients for Diabetic Retinopathy and has identified 50 of them who are eligible for treatment.
“I am proud to be a part of this project. Because of this project, many patients in my centre now know about diabetes and how it affects the eyes. This is one of the most useful programmes for the people in rural areas. Through this project, I too have learned about DR and to capture fundus images. Although the treatment for DR is free of cost, the challenge is to make the people to go for regular follow-up and treatment.
This project has made patients with diabetes in my centre aware about DR, and its prevention and treatment. I thank the project, Aravind Eye Hospital and Government of Tamil Nadu for this wonderful initiative.
- Case Study: A Doctor’s Tale
Dr Venugopal is the head of Retina-Vitreous Services at Aravind Eye Hospital, Tirunelveli. He started his career at Aravind Eye Hospital as a medical officer in 2010 and rose to become a consultant in 2012. He has published papers in 10 international journals so far. His areas of interest are vitreo-retinal diseases and ocular trauma/infections/inflammation/paediatric retina.
Dr Venugopal is part of the DR project and helped to screen and treat many patients for DR. He has trained ophthalmologists and general physicians in fluorescein angiography and optical coherence tomography as part of the Trust DR programme.
“I am glad to contribute my knowledge in capacity building of physicians and ophthalmologists as part of the Trust project. I also wish that there were more LASER treatment options for the Diabetic Retinopathy patients in Tirunelveli district. Such a self-sustainable model would help the government health system to cater for the needy people.
As a member of Aravind Eye Care System, I thank the QEDJT for providing me such a rare opportunity in my career to share my learning with others. Scaling up of this project to all parts of the country can help save many from going blind in India.”





