


Policy Brief – Control of Retinopathy of Prematurity in India
ROP is a major cause of blindness in children in many middle-income countries including India


Prevention of blindness from ROP requires collaborative efforts from all government and
other agencies
A strong policy framework is the need of the hour to prevent infants going blind from ROP
The problem
Retinopathy of prematurity (ROP) is a potentially blinding eye condition which affects infants born preterm. Babies born at or before 34 weeks gestational age (i.e., six or more weeks preterm) or weighing less than 2000gms at birth, are at greatest risk. ROP is a major cause of blindness in children in many middle-income countries and is becoming an increasingly important cause in India, as neonatal services expand and more preterm babies survive.
ROP was first described almost 80 years ago and the risk factors are also well known i.e., low gestational age, inadequately monitored supplemental oxygen from immediately after birth, infection and failure to gain weight after birth. Clinical trials have also clearly demonstrated that urgent laser treatment for the sight-threatening stages of ROP is very effective at preserving vision.
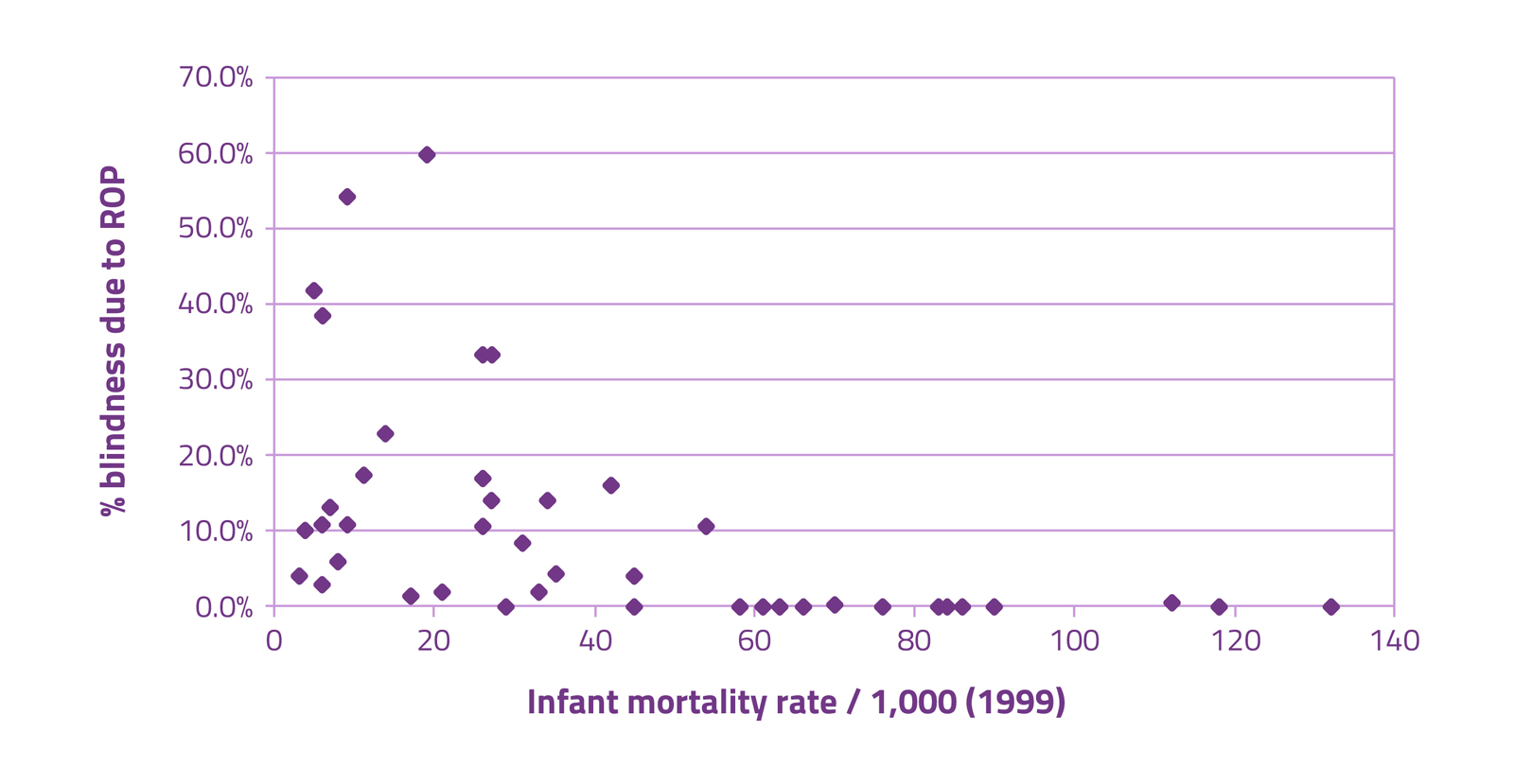
Studies show that countries with infant mortality rates (IMRs) in the range 9-60/1000 live births are the most affected. In countries with high IMRs, most preterm infants do not survive. At the other end of the spectrum, countries with very low IMRs have low rates of ROP blindness as neonatal care services are of high quality and ROP screening and treatment services are available.
As a result of concerted efforts to reduce infant and child mortality in India, the IMR is falling (28/1000 live births in 2015), but blindness from ROP is increasing. India has the highest number of preterm births – 3.5 million annually in 2010. Recent estimates of visual impairment and blindness due to ROP suggest that 10% of the 32,300 infants affected globally (in 2010) were born in India. The expanding provision of neonatal care services in India means that the number of preterm infants at risk of blindness from ROP will continue to increase. A conservative estimate suggests that up to 18,000 infants will go blind every year in India unless control is scaled up.
Unfortunately, regular ROP screening programmes are not mandatory for neonatal intensive care units in India, including in Sick Newborn Care Units which are being scaled up across India. However, screening for ROP is included in the Government’s RBSK programme.


Proportion of blindness due to ROP, by Infant Mortality Rate for the year 1999
The impact
Blindness from ROP has economic, legal and social implications for affected children and their families, governments and civil society. For example, in 2015 the Supreme Court of India ordered Tamil Nadu State Government to compensate INR 1.8 crores to a 18-year-old girl who lost her vision from ROP in a medical negligence case against a government-run hospital. Another hospital was ordered to pay INR 68 Lakhs for another child. Providing services for the prevention, detection and treatment of ROP is, therefore, financially and legally prudent.
A recent study from India, in which parents of ROP blind children were interviewed, powerfully illustrated the impact on families. Many parents experienced social isolation and most were concerned about the future of their child. Most had borrowed money or sold assets to pay for treatment, and several marriages had come under intolerable pressure.
The strategies required for control
- Prevention of preterm birth, which is challenging, but could include regulation of assisted fertilization practices, by limiting the number of fertilized embryos implanted;
- Antenatal steroids for all threatened preterm deliveries, which reduce many of the complications of preterm birth, including ROP; High quality neonatal care for preterm infants from immediately after birth, to control the known risk factors;
- High coverage of weekly ROP screening by ophthalmologists in neonatal units, or in eye units or District Early Intervention Centres for babies who have been discharged from neonatal care, to detect infants with the sight-threatening stages. Screening can also be undertaken by trained technicians using wide-field digital cameras, supported by an ROP expert ophthalmologist;
- Urgent laser treatment of sight-threatening ROP by skilled ophthalmologists;
- Long-term follow up to detect and manage the eye complications of preterm birth and ROP;
- Empowering ASHA workers and ANMs to ensure mothers threatening preterm delivery give birth in facilities with a neonatal unit, and counselling mothers of preterm infants of the need for screening for ROP and for long-term follow up.
- Strengthen at least one tertiary eye care department in each State as an ROP centre of excellence.

Ophthalmologist examining a preterm baby for ROP in Cuttack, India

Abdullah, aged 16, continues to have regular eye examinations by Dr. Subhadra Jalali who has seen Abdullah grow up since he was only a few weeks old
Scaling up services for ROP in India
Scalable and effective initiatives to improve neonatal care and for ROP screening and treatment and are urgently required to prevent blindness from ROP. The Queen Elizabeth Diamond Jubilee Trust is supporting senior neonatologists in AIIMS, New Delhi and PGIMER, Chandigarh to build capacities of neonatal teams to reduce the risk of ROP in medical colleges and 22 district SCNUs in four States across India. Public-private partnerships are also being supported to build the capacities of local ophthalmologists in ROP screening and treatment in the same facilities.
The cost of setting up a ROP screening and treatment program in a cluster based on the Trust-supported program (i.e., in one medical college neonatal unit and 4 SNCUs in neighbouring districts) is approximately Rs 40,00,000 per cluster, with annual running costs of Rs 60,000 per cluster. A recent study in Brazil estimated that the incremental cost of integrating screening and treatment for ROP was less than 1% of the cost of providing neonatal care.
A study in Mexico and the USA estimated the costs to families of raising a blind child, and the lost productivity of carers and ROP blind individuals. These costs were considerable in both countries: in Mexico and the USA the incremental net annual monetary benefit of providing a service to prevent blindness from ROP was $206,574,333 and $205,906,959 respectively.
The WHO/UNICEF initiative Every Newborn: An Action Plan to End Preventable Deaths, states that “a healthy society is one in which women and adolescent girls, newborns and children survive and thrive.” The same applies to children who are born preterm.
![]()
TORs and Minutes of Task Force
Constitution of National Taskforce on prevention of blindness from Retinopathy of Prematurity with following terms of reference (Nirman Bhavan, New Delhi, September 2014)
Terms of Reference
- National taskforce on prevention of blindness from Retinopathy of Prematurity
- Support further development of evidence base on ROP to inform the strategy
- Provide advice for policy makers on the best ways of government investment in prevention of blindness from ROP
- Provide guidance to strengthen ROP screening and management services
- Provide advice to government on options for better integration of ROP services in to NHM
- Support the development of inter-departmental and multi-sectorial partnerships for ROP
- Priorities for Control
- Focus on improving neonatal care to reduce the risk of ROP
- Sensitization of professionals
- Integrate detection of ROP into existing programmes i.e. NCPB; SNCUs and RBSK wherever possible, by building capacity and/or referrals
- Build capacity for treatment
- Monitoring and Evaluation Indicators
- Advocacy leads to new policy, change in existing policy and new guidelines
- Strengthening health systems: improved survival rates of preterm infants without severe ROP
- Greater access to services: number of SNCUs/neonatal units with new ROP programmes
- Greater provision of services: number and proportion of eligible infants screened and the proportion treated according to protocols
- Creating awareness among obstetricians in workshops/conferences for obstetricians/ midwives/TBAs/nurses: four main messages:
- Risks to vision associated with preterm birth
- Promote NNF/standard guidelines for resuscitation of preterm infants
- Promote use of antenatal steroids among mothers at risk of preterm pregnancy and give all four doses recommended
- Communicate with parents of preterm infants about the need for timely retinal examination
- Operational guidelines for Trust-supported State programmes
- Improving the quality of neonatal care to reduce the risk of severe ROP
- Competency based training for ophthalmologists (screening and treatment) and technicians (screening) and nurses
- Protocols for examination, treatment and follow up
- Online data collection for ROP and Modification of UNICEF database for monitoring rates of severe ROP
- Based on the situational analysis findings the Task Force has selected two states, i.e. Madhya Pradesh and Telangana, for implementation of the model ROP programme in Phase I, and three more states, i.e. Maharashtra, Odisha and Rajasthan, for implementation in Phase II
- Usage of CPAP & Blenders in SNCUs – Early usage of CPAP should be encouraged for prevention of ROP. CPAP machines are available in most of the SNCUs but there is a need for training to the SNCU staff in usage of CPAP
- FOGSI will be provided with a one page note on ‘the role of an obstetrician in prevention of ROP’ and that will be shared with the professional groups as part of the conference material in the next FOGSI conference
- Indian Journal of Paediatrics will release a special issue on ROP, shortly
- A discussion was initiated on whether ROP screening should be combined with comprehensive eye examination under RBSK
- Screening should have high sensitivity and so the criterion for screening will be – any baby born at or below 36 weeks gestation and with less than 2000 gram birth weight
- The Technical Expert Group working on ‘Competency based training in screening and management of ROP’ has prepared training curricula based on CANMEDS framework
- The Technical Expert Group working on ‘Capacity building of neonatologists and their teams for prevention of avoidable blindness from ROP’ has prepared training curricula emphasizing on 5 domains – 1. Optimizing oxygen usage, 2. Less exposure to blood products, 3. Reducing infections, 4. Improving nutritional status and 5. Good developmental support
- A systematic review of National guidelines of different countries is to be done and the findings can be adapted to India and incorporated in National ROP guidelines
- Dr. Renu Srivastava has been working on ‘inclusion of ROP-related fields and indicators into GOI-SNCU database’
- Comprehensive guidelines on the eye conditions covered by RBSK have been produced and circulated. The background and purpose of the guidelines were explained, highlighting that the guidelines can and will be modified
- Competency based training in screening and treatment. Separate sub-tasks were identified for screening and for treatment, and then the CANMEDS framework was used to identify the competencies required for each task under the following domains:
- Expert (clinical skills)
- Communicator
- Collaborator
- Health Advocate
- Scholar
- Professional
- The next step will be to develop the assessments for each competency which will need to be tested to ensure they are feasible to implement. The content of training can then be finalized
- M&E: The number of infants developing Stage 4 and 5 ROP in Trust supported SNCUs/NICUs needs to be reported
- Training: Safety to specifically included in the competency based training framework
- Advocacy: Compile and publish data on increasing ROP blindness in India; And establish a national register of Stage 4 / 5 so that output is just number affected
- Model programmes: Undertake situation analysis in Chhattisgarh to consider as the next State. Use commitment by Medical College ophthalmologists and paediatricians as a critical criteria for expansion
- Responding to media / other issues: PHFI to formerly set up a small communication group to co-ordinate responses to unfavourable articles in the media etc., so that responses are appropriate and do not come from individuals
- Collaboration: Ensure that the National ROP Task Force is represented at Child Health policy meetings
Operational Guidelines
Retinopathy of Prematurity (ROP) is a potentially blinding disease of the eye that can affect infants born four or more weeks preterm and receive intensive neonatal care. In ROP, the developing retinal blood vessels grow abnormally, which can lead to detachment of the retina and total blindness, usually in both eyes. The risk of severe sight-threatening ROP, which is higher in more preterm infants, can be reduced by quality improvement measures which reduce exposure to known risk factors such as poorly administered supplemental oxygen, sepsis and poor weight gain after birth. Early detection of sight-threatening ROP (ST-ROP), followed by urgent laser treatment, is highly effective in preserving the sight of babies.
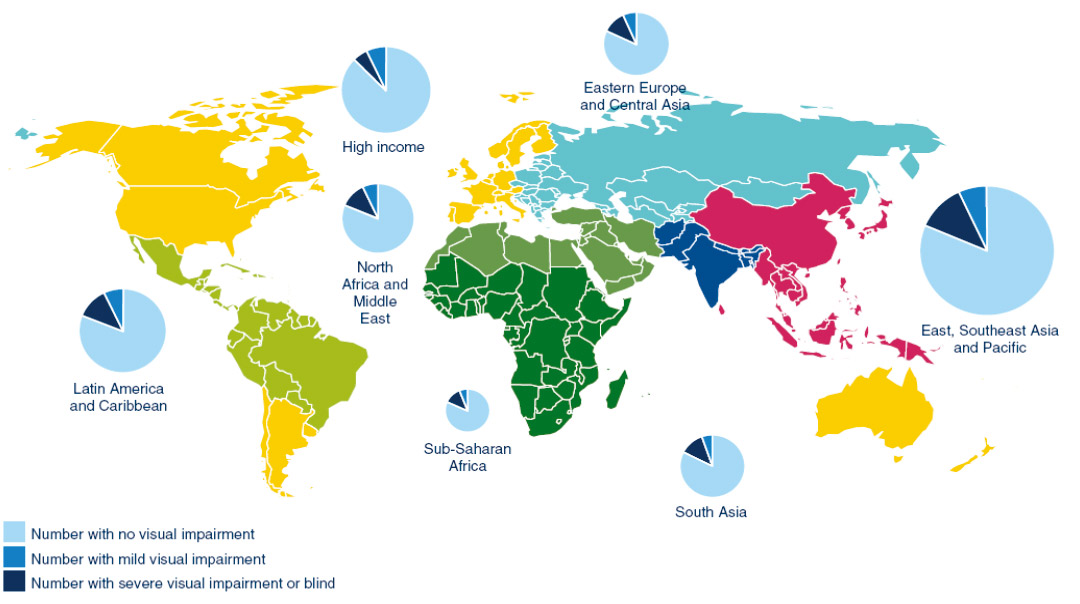
Recent estimates show that 32,000 infants became blind or visually impaired from ROP every year world-wide, being a far higher estimate that 10 years ago. Most of the ROP-blind infants were born in countries in Asia.
Distribution of ROP and its effects across the globe
ROP National Taskforce TORs & TEGs
Terms of Reference for Technical Experts Group on Advocacy & Communication for Prevention of Sight-Threatening ROP
- Assess and review existing government policies, Government Orders/Directive Orders and identify gaps for advocacy
- Review and finalize draft advocacy plan developed by PHFI for the Trust and amend as necessary
- Suggest advocacy materials as required for the strategy
- Review existing education materials for parents regarding ROP. Modify and translate as necessary
- Help develop a resource kit for different audiences
- Work with The Trust to develop a strategy to communicate learning from The Trust’s programme for ROP
- Periodically assess the progress towards identified activities and stated timelines
- Meet periodically to develop the strategy and to monitor progress
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Dr. Usha Raman | Professor, Department of Communication | University of Hyderabad |
| Dr. Subhadra Jalali | Director, Newborn Eye Health Alliance (NEHA), Director- Quality | LV Prasad Eye Institute, Hyderabad |
| Dr. Bijoy Patro | Department of Pediatrics | Lady Hardinge Medical College, New Delhi, India |
| Dr. Srinivas Murki | Consultant Neonatologist; NICU (Neonatal Intensive Care Unit) - In Charge | Fernandez Hospitals, Hyderabad |
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Pulic Health Hyderabad |
| Dr. Tripura Batchu | Programme Coordinator | Indian Institute of Pulic Health Hyderabad |
| Prof. Clare Gilbert | Technical Advsor/ Professor, Co-Director ICEH, London UK | London School of Hygiene & Tropical Medicine, London UK |
| Ms. Gina Sharma | Communications Officer | Public Health Foundation of India, New Delhi |
| Ms. Kavita Chauhan | Health Communication Division | Public Health Foundation of India, New Delhi |
| Ms. Hema Bhogaraju | CVR Health (TV Channel) | |
| Ms. Akanksha Nigam | Research Assistant, Communications | Indian Institute of Pulic Health Hyderabad |
Terms of Reference for Technical Experts Group on Capacity Building of Neonatologists
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Dr. Ashok Deorari | Professor & Head | Department of Pediatrics, All India Institute of Medical Sciences, New Delhi |
| Dr. Anu Thukral | Assistant Professor | Department of Pediatrics, All India Institute of Medical Sciences, New Delhi |
| Dr. Deepak Chawla | Professor - Neonatology | Department of Neonatology-Pediatrics, Government Medical College & Hospital, Chandigarh |
| Dr. Praveeen Kumar | Professor - Neonatology | Department of Pediatrics, Post Graduate Institute of Medical Education & Research, Chandigarh |
| Dr. Parijat Chandra | Additional Professor - Ophthalmology | Department of Ophthalmology, All India Institute of Medical Sciences, New Delhi |
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Public Health Hyderabad |
| Prof. GVS Murthy | Director | Indian Institute of Public Health Hyderabad |
| Dr. Sunil | Neonatologist | National Neontology Forum, India |
| Prof. Clare Gilbert | Technical Advisor/ Professor, Co-Director ICEH, London UK | London School of Hygiene & Tropical Medicine, London UK |
| Dr. Mangat Dogra | Professor & Head of Ophthalmology | Department of Ophthalmlogy, Advance Eye Care Centre, Post Graduate Institute of Medical Education & Research, Chandigarh |
Terms of Reference for Technical Experts Group on Capacity Building of Ophthalmologists by Training in the Detection and Management of ROP
- Delineate the capabilities needed, clinical and non-clinical, by ophthalmologists and neonatologists for case detection, and for treating sight threatening ROP both in the short term (during Trust programme) and the long term (beyond the Trust programme)
- Develop learning objectives, competency-based curricula, and assessment methods
- Review residency training curriculum for ophthalmologists and suggest changes, to be taken forward through advocacy
- Make recommendations regarding criteria required by training institutions e.g. volume of cases examined and treated
- Periodically assess the progress towards identified activities and stated timelines
- Meet periodically to develop the strategy and to monitor progress
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Dr. Subhadra Jalali | Director, Newborn Eye Health Alliance (NEHA), Director - Quality | LV Prasad Eye Institute, Hyderabad |
| Dr. Narendran Venkatapthy | Chief Medical Officer | Aravind Eye Hopital, Coimbatore |
| Dr. Pramod Bhende | Director | Sankara Nethralaya, Chennai |
| Dr. Anand Vinekar | Professor & Head - Pediatric Retina Department | Narayana Nethralaya, Bangalore |
| Dr. Sai Kiranmayee | Vitreo-Retinal Specialist | Pushpagiri Vitreo Retinal Institute, Hyderabad |
| Dr. Raghupathy Anchala | Associate Professor | Indian Institute of Public Health Hyderabad |
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Public Health Hyderabad |
| Prof. GVS Murthy | Director | Indian Institute of Public Health Hyderabad |
| Prof. Clare Gilbert | Technical Advisor/ Professor, Co-Director ICEH, London UK | London School of Hygiene & Tropical Medicine, London UK |
| Dr. Venkata Rao. K |
Terms of Reference for Technical Experts Group on HMIS, IT
- Help to design data management tools required for M&E
- Review the developed HMIS framework for M&E
- Periodically review the progress of data collection of the monitoring indicators developed in the HMIS frame work
- Formulate TOR for midterm & final evaluation
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Mr. RD Thulasi Raj | Director - Operations; Executive Director- LAICO | Aravind Eye Care System; Lions Aravind Institute of Community Ophthalmology (LAICO) |
| Dr. Srinivas Murki | Consultant Neonatologist; NICU (Neonatal Intensive Care Unit) - In Charge | Fernandez Hospital, Hyderabad |
| Dr. Venkata Rao | ||
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Public Health Hyderabad |
| Dr. Anand Vinekar | Professor & Head - Pediatric Retina Department | Narayana Nethralaya, Bangalore |
| Mr. Ganesh Babu | ||
| Prof. GVS Murthy | Director | Indian Institute of Public Health Hyderabad |
| Dr. Raghupathy Anchala | Associate Professor | Indian Institute of Public Health Hyderabad |
Terms of Reference for Technical Experts Group on National Guidelines
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Dr. Arun Singh | National Advisor - Rashtriya Bal Swasthya Karyakram (RBSK) | Ministry of Health & Family Welfare, Government of India, New Delhi |
| Dr. Renu Srivastava | Sick Newborn Care Units (SNCUs) Coordinator, Childhealth | Ministry of Health & Family Welfare, Government of India, New Delhi |
| Dr. RV Azad | Senior Advisor | ROP (Retinopathy of Prematurity) National Task Force |
| Dr. Ashok Deorari | Professor & Head | Department of Peadiatrics, All India Institute of Medical Sciences, New Delhi |
| Prof. Clare Gilbert | Technical Advisor/ Professor, Co-Director ICEH, London UK | London School of Hygiene & Tropical Medicine, London UK |
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Public Health Hyderabad |
| Dr. Parijat Chandra | Additional Professor - Ophthalmology | Department of Ophthalmology, All India Institute of Medical Sciences, New Delhi |
| Dr. Mangat Dogra | Professor & Head of Ophthalmology | Department of Ophthalmlogy, Advance Eye Care Centre, Post Graduate Institute of Medical Education & Research, Chandigarh |
| Dr. Anand Vinekar | Professor & Head - Pediatric Retina Department | Narayana Nethralaya, Bangalore |
| Dr. Subhadra Jalali | Director, Newborn Eye Health Alliance (NEHA), Director - Quality | LV Prasad Eye Institute, Hyderabad |
| Dr. Pranab Das | Consultant Vitreo-Retina Surgeon | Calcutta Medical Research Institute, Kolkata, India |
Terms of Reference for Technical Experts Group on Programme Planning & Review of Proposals
- Review Operational Guidelines developed for Trust supported programmes
- Review proposals received from mentoring partners
- Support development of State level models
- Provide technical input to mentoring partners
- Meet periodically to assess need for technical input
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Dr. Ajay Khera | Deputy Commissioner - Child Health | Ministry of Health & Family Welfare, Government of India, New Delhi |
| Dr. Ashok Deorari | Professor and Head | Department of Pediatrics, All India Institute of Medical Sciences, New Delhi |
| Dr. Promila Gupta | Principal Consultant; Former Deputy Director General National Programme for Control of Blindness (NPCB) (Retired) | Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India, New Delhi |
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Public Health Hyderabad |
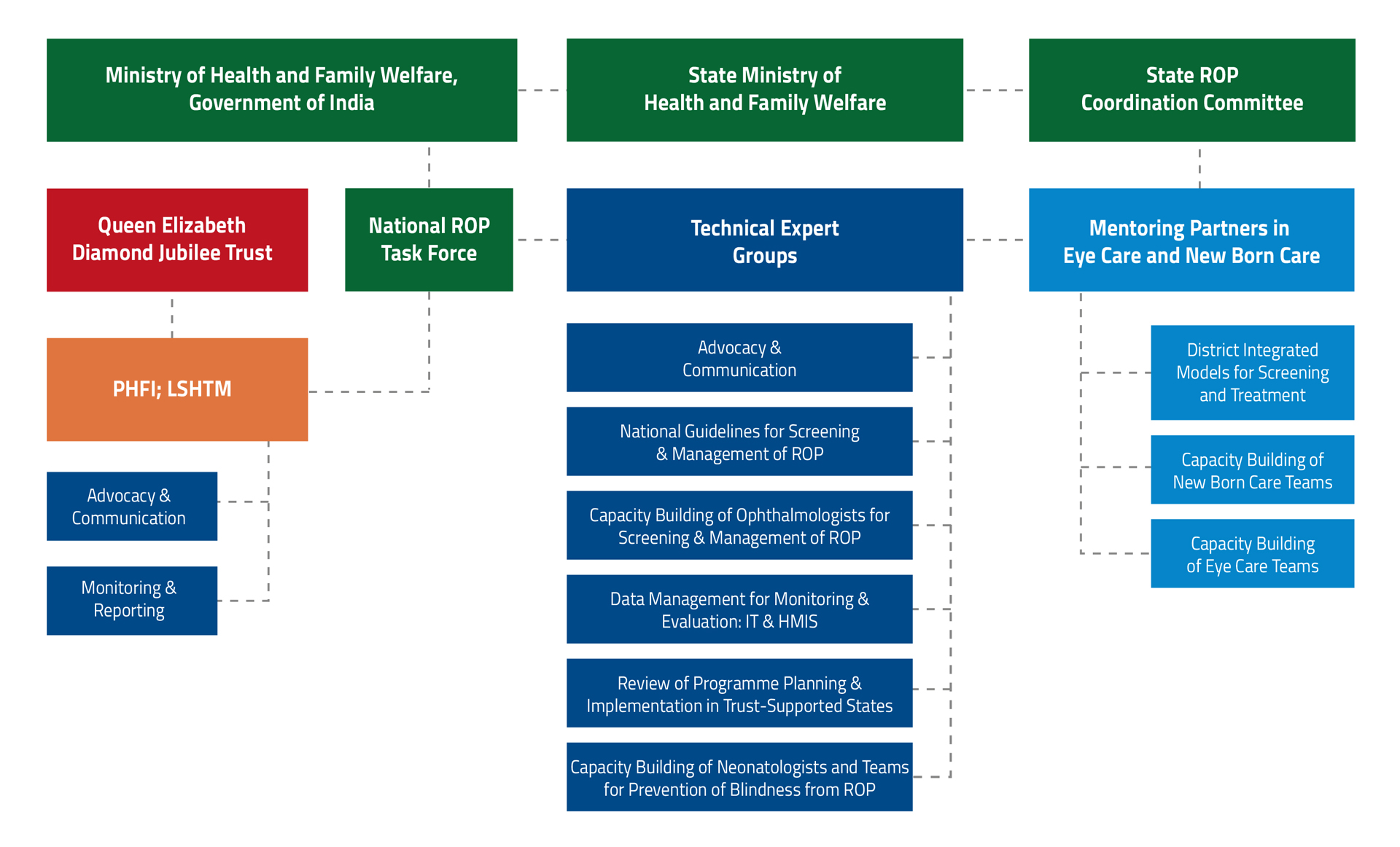
Governance Structure
Links to Training Institutions under the Project
| Hospital | Type of Mentoring | Website | Address |
|---|---|---|---|
| PVRI Hyderabad | Eye Care | Pushpagiri Vitreo Retina Institute, Plot No 241, Uma Plaza, 9, West Marredpally, Secunderabad, Telangana 500026 | |
| LVPEI Hyderabad | Eye Care | L V Prasad Eye Institute, Kallam Anji Reddy Campus, LV Prasad Marg, Opp. PVR, Park View Enclave, Banjara Hills, Hyderabad, Telangana 500034 | |
| Fernandez Hospitals | Neonatal Care | 3-6-282, Hyderguda-Basheerbagh Rd, AP State Housing Board, Hyderguda, Hyderabad, Telangana 500029 | |
| Post Graduate Institute of Medical Education & Research | Eye Care, Neonatal Care and QI team | Sector-12, Chandigarh, Pin- 160 012 Chandigarh | |
| LVPEI Bhubaneshwar | Eye Care | LV Prasad Eye Institute, Mithu Tulsi Chanrai Campus, Patia Rd, Bhubaneswar, Odisha 751024 | |
| Capital Hospital | Neonatal Care | Capital Hospital, Udyan Marg, Unit 6, Ganga Nagar, Bhubaneswar, Odisha 751020 | |
| HV Desai Eye Hospital | Eye Care | 93, Katraj-Hadapsar Bypass Rd, Tarawade Vasti, Mohammed Wadi, Pune, Maharashtra 411060 | |
| KEM Hospital, Pune | Neonatal Care | 489, Sardar Moodliar Road, Rasta Peth, Pune, Maharashtra 411011 | |
| AIIMS, New Delhi | QI team | All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110029 | |
| GMCH Chandigarh | QI team | Government Medical College & Hospital, Sector 32, Chandigarh, Pin 160030 |
Case Studies
On 2 February 2017, baby Naveena and her twin sister Radha were born prematurely at District Hospital, Nalgonda in Telangana. Born at 28 weeks of gestation, Radha one of the twins died due to complications. On the fifth day of their birth, the mother who was HIV positive died due to post-partum haemorrhage.
Baby Naveena weighed one kg when her mother died. Unable to deal with his wife’s death, Naveena’s father abandoned her and never came back. The dedicated SNCU staff and the head of the SNCU unit Dr Yadaiah took utmost care of baby Naveena and made sure she was alive. One big sigh of relief to the SNCU team was Naveena’s blood report was found negative for HIV.
Over the days Saritha, a 26 year old mother of two children who is also part of the support staff at Nalgonda SNCU took charge of Naveena. She gave her Kangaroo Mother Care (KMC) support for 6 hours a day. Along with KMC other lifesaving interventions were also used; a sound spa that enabled her to develop sense of hearing, a water bed to prevent bed sores and a wrist device tied to her arm to detect hypothermia. Expressed breast milk (EBM) network, an effective innovation helped Naveena have access to breast milk donated by other mothers. With the love and compassion from SNCU Nalgonda team Baby Naveena gained significant weight. Dr Chandu who was ROP specialist at Nalgonda District Hospital used to check on her at regular intervals.
Naveena’s story clearly demonstrates that practising quality neonatal care (POINTS – Pain control, Optimal oxygenation, Infection control, Nutrition interventions, Temperature control and Supportive care) with strict adherence to protocols can not only help babies survive but thrive as well. These interventions reduce the incidence of ROP from 47.2% to 22.7% (according to an experience from NICU in Northern India).
Naveena’s story is being covered widely in magazines to generate motivation and inspiration among healthcare providers, also to spread awareness about impact of quality improvement in care provision at SNCUs.

Collaboration of PHFI, under the Trust supported ‘Retinopathy of prematurity programme’, with District Hospital, Nalgonda; Fernandez Hospital and LV Prasad Eye Institute, protected the life and sight of an underprivileged girl baby
Baby Rishita is a girl child born in 28th week of gestation with 650 grams birth weight, on 30th December 2015. Her parents live in Perika Kondaram village, where female infanticide is a major social problem. The village is about 70 Km from the district headquarters, i.e Nalgonda Town and about 35 Km from the nearby small town, i.e. Nakrekal. The village doesn’t have provision for public transport and the people depend on private auto rickshaws for transport, which are also very few. The parents of the baby are college dropouts and working as agriculture labourers. The family belongs to Scheduled Caste, doesn’t have their own farm, but have few sheep.
Rishita’s mother suffered from hypertension during pregnancy and had eclampsia before delivery. At 28 weeks pregnancy she had to undergo caesarean section in a private nursing home. She was hospitalized in a private nursing home for 9 days and bed ridden for about three weeks after her discharge from Hospital. About one lakh of out of pocket expenditure for her treatment during and after delivery, left the family in debts.
The private nursing home refused to admit the 650 grams baby as there was no hope on its survival. Then the relatives admitted Rishita in Nalgonda District Hospital. Nalgonda District Hospital is the only nearby government hospital, where there is a Sick newborn care unit.
Nalgonda District Hospital is a government hospital, has well equipped Sick Newborn Care Unit (SNCU), with a dedicated team of four well trained paediatricians and 12 nurses. Initially even this team had no hope on the baby until when it began to show positive signs. “I really had some belief that she could survive, when she was holding my finger” said Dr. Yadaiah, the in charge of the SNCU. Gradually this baby became ‘special’ to them. One of the doctors of the team came to know about using ‘sound spa’ as part of management of his grandson, who was also born premature and treated by doctors in USA. They got a ‘sound spa’ from the United States and used for this baby to have her hear different sounds of the world, which she would have heard from her mother’s womb, had she not born too early. Dr. Khadar Jilani expressed that there had been a bond among the baby and the hospital staff – “We were talking to the baby regularly”. They dedicated one sister in each shift for the baby.
The mentors of ‘the Trust supported model ROP programme’ in the State, Dr. Srinivas Murki from neonatology department of Fernandez Hospital, Hyderabad and Dr. Subhadra Jalali, retina specialist from LV Prasad Eye Institute, Hyderabad visited the unit frequestly and provided their support and guidance to the health care team of the unit. First screening for ROP was done at day 25 of birth of the baby, by the in-house ophthalmologist Dr. K. Chandu, who suspected retinopathy of prematurity (ROP). Dr. Subhadra Jalali noticed the need for a laser surgery to prevent blindness from retinopathy of prematurity. It was then; a laser surgery was performed, for the first time, in the SNCU in Nalgonda.
The mother expressed her gratitude towards the doctors, said that – doctors provided medicines for the baby and food and accommodation for mother. She said, “Dr. Yadaiah told that the vessels in the baby’s eyes were not developed accordingly and if regular eye check-up is not done it would gradually go into blindness.” The baby underwent laser treatment for ROP twice. Later on, before discharge of the baby, after screening for ROP the mother was told that the baby’s eyes were normal and there would be no problem.
The baby, of 1700 grams weight, was discharged from the hospital on April 29, 2016. As suggested by the hospital, the mother was ready to take the baby to hospital for monthly follow-up check-ups.

Dr Srinivas Murki, Newborn Care Mentor with baby Rishita

Rishita benefits from the use of a Sound Spa

Dr Subhadra Jalali, Eye Care Mentor, looks after baby Rishita

Tiny Rishita holds the finger of Dr Yadaiah, paediatrician in Nalgonda DH
One of twin preterm babies of Sneha Kalokhe was referred from the district hospital (DH) in Nanded, a town over 400 km from Pune to it’s DH Neonatal Intensive Care Unit (NICU) for severe ROP. The preterm baby was treated successfully by the team from H V Desai Eye Hospital on 10th June 2017.
Sneha’s husband Bhimrao Kalokhe is a 28 year old young gentleman residing in remote village near Nanded district. He comes from poor socioeconomic background and works as a farm labrourer. He studied upto high school and then dropped out owing to family’s financial difficulties. His family of five (old parents, wife and a 5 year old daughter) are dependent on his meager daily earning of Rs. 300 (approximately 4.6 USD) per day. There are some days when there would be no farming which would be no work for Bhimrao.
Despite their poverty, the parents’ joy knew no bounds when they came to know of the twin pregnancy. Sneha, the mother went for regular antenatal care visits during the pregnancy but delivered prematurely at 33 weeks. She delivered in a private hospital and both the babies fell sick right after birth.
The twins weighed 1600 and 1700 grams respectively and doctors informed the parents that babies would require, oxygen and ventilation. They were admitted in the Neonatal Intensive Care Unit of the same hospital but the bill went up to Rs 56000 (USD 875) within a week. The family simply didn’t have money to pay the hospital or have any assets to sell. Thankfully their extended family came to their rescue and helped them pay the hospital bill. The parents were then forced to shift the twins to a government hospital where they could get free care.
Bhimrao was by the side of his wife for few days but could not afford to lose his income hence he had to leave his wife alone while the babies were being taken care in the SNCU. During that period the family was so short of money that sometimes they had to starve for a day or two. To add to their difficulties, Sneha got acute gastroenteritis during that period and had to be hospitalized adding to their financial burden.
Dr Chavan (paediatrician) from Nanded DH referred them to Dr Ghonsikar (ophthalmologist) for ROP screening. Dr Ghonsikar, a private practitioner who screens for ROP at Nanded DH noticed that one of the twins had severe ROP. Entire world came crashing down for the husband and wife when the ophthalmologist told them that both babies had ROP and could go blind if not treated on time. Both Sneha and her mother started crying. After so much of physical and emotional stress, they had to face another harsh reality.
The DH in Nanded did not have the facility to treat ROP in pre-term infants and the treatment was available only in few private hospitals. The parents could not afford to pay for the treatment in private hospitals and were advised to travel to Pune for the treatment. As laser treatment is expensive in private hospitals, Dr Ghonsikar referred them to DH Pune where free treatment could be availed. They chose to travel by train, a seven hour long journey with the newborn babies.
Dr Ashwini Sonawne, ophthalmologist from H V Desai Eye Hospital, went to Pune DH and performed laser on one of the twins who had severe ROP. When Dr Ashwini explained to them about need for follow up, parents readily agreed to stay in Pune for a week. During this stay, parents had to stay and sleep on the road as they could not afford to pay for a place to stay. Three adults had to share a meal of 2 Rotis (Indian bread) twice a day which Sneha was entitled to. They had no money to buy food.
Despite these hardships, they showed their utmost commitment for the welfare of their children and came back to H V Desai Hospital for follow up after a week. Dr Devika (neonatologist at Pune DH) and Dr Sirsikar (ophthalmologist) were kind enough to arrange free transport for follow up visit.
Parents were delighted to know that their baby’s ROP had started regressing and agreed to keep regular follow up with local ophthalmologist after going back to Nanded. They would also come back to Pune for follow up if advised by local ophthalmologist.
Coming to Pune proved a blessing in disguise for the family. Here they received all the support and counselling and free laser treatment for their child. Before leaving they thanked the H V Desai team and Pune DH for saving their daughter from going blind permanently.
* Name has been changed

Sneha Kalokhe with her twin babies, mother and husband at HV Desai Hospital, Pune, India

Laser in progress for Sneha’s baby at HV Desai Hospital, Pune, India
- Naveena
On 2 February 2017, baby Naveena and her twin sister Radha were born prematurely at District Hospital, Nalgonda in Telangana. Born at 28 weeks of gestation, Radha one of the twins died due to complications. On the fifth day of their birth, the mother who was HIV positive died due to post-partum haemorrhage.
Baby Naveena weighed one kg when her mother died. Unable to deal with his wife’s death, Naveena’s father abandoned her and never came back. The dedicated SNCU staff and the head of the SNCU unit Dr Yadaiah took utmost care of baby Naveena and made sure she was alive. One big sigh of relief to the SNCU team was Naveena’s blood report was found negative for HIV.
Over the days Saritha, a 26 year old mother of two children who is also part of the support staff at Nalgonda SNCU took charge of Naveena. She gave her Kangaroo Mother Care (KMC) support for 6 hours a day. Along with KMC other lifesaving interventions were also used; a sound spa that enabled her to develop sense of hearing, a water bed to prevent bed sores and a wrist device tied to her arm to detect hypothermia. Expressed breast milk (EBM) network, an effective innovation helped Naveena have access to breast milk donated by other mothers. With the love and compassion from SNCU Nalgonda team Baby Naveena gained significant weight. Dr Chandu who was ROP specialist at Nalgonda District Hospital used to check on her at regular intervals.
Naveena’s story clearly demonstrates that practising quality neonatal care (POINTS – Pain control, Optimal oxygenation, Infection control, Nutrition interventions, Temperature control and Supportive care) with strict adherence to protocols can not only help babies survive but thrive as well. These interventions reduce the incidence of ROP from 47.2% to 22.7% (according to an experience from NICU in Northern India).
Naveena’s story is being covered widely in magazines to generate motivation and inspiration among healthcare providers, also to spread awareness about impact of quality improvement in care provision at SNCUs.
- Rishita
Collaboration of PHFI, under the Trust supported ‘Retinopathy of prematurity programme’, with District Hospital, Nalgonda; Fernandez Hospital and LV Prasad Eye Institute, protected the life and sight of an underprivileged girl baby
Baby Rishita is a girl child born in 28th week of gestation with 650 grams birth weight, on 30th December 2015. Her parents live in Perika Kondaram village, where female infanticide is a major social problem. The village is about 70 Km from the district headquarters, i.e Nalgonda Town and about 35 Km from the nearby small town, i.e. Nakrekal. The village doesn’t have provision for public transport and the people depend on private auto rickshaws for transport, which are also very few. The parents of the baby are college dropouts and working as agriculture labourers. The family belongs to Scheduled Caste, doesn’t have their own farm, but have few sheep.
Rishita’s mother suffered from hypertension during pregnancy and had eclampsia before delivery. At 28 weeks pregnancy she had to undergo caesarean section in a private nursing home. She was hospitalized in a private nursing home for 9 days and bed ridden for about three weeks after her discharge from Hospital. About one lakh of out of pocket expenditure for her treatment during and after delivery, left the family in debts.
The private nursing home refused to admit the 650 grams baby as there was no hope on its survival. Then the relatives admitted Rishita in Nalgonda District Hospital. Nalgonda District Hospital is the only nearby government hospital, where there is a Sick newborn care unit.
Nalgonda District Hospital is a government hospital, has well equipped Sick Newborn Care Unit (SNCU), with a dedicated team of four well trained paediatricians and 12 nurses. Initially even this team had no hope on the baby until when it began to show positive signs. “I really had some belief that she could survive, when she was holding my finger” said Dr. Yadaiah, the in charge of the SNCU. Gradually this baby became ‘special’ to them. One of the doctors of the team came to know about using ‘sound spa’ as part of management of his grandson, who was also born premature and treated by doctors in USA. They got a ‘sound spa’ from the United States and used for this baby to have her hear different sounds of the world, which she would have heard from her mother’s womb, had she not born too early. Dr. Khadar Jilani expressed that there had been a bond among the baby and the hospital staff – “We were talking to the baby regularly”. They dedicated one sister in each shift for the baby.
The mentors of ‘the Trust supported model ROP programme’ in the State, Dr. Srinivas Murki from neonatology department of Fernandez Hospital, Hyderabad and Dr. Subhadra Jalali, retina specialist from LV Prasad Eye Institute, Hyderabad visited the unit frequestly and provided their support and guidance to the health care team of the unit. First screening for ROP was done at day 25 of birth of the baby, by the in-house ophthalmologist Dr. K. Chandu, who suspected retinopathy of prematurity (ROP). Dr. Subhadra Jalali noticed the need for a laser surgery to prevent blindness from retinopathy of prematurity. It was then; a laser surgery was performed, for the first time, in the SNCU in Nalgonda.
The mother expressed her gratitude towards the doctors, said that – doctors provided medicines for the baby and food and accommodation for mother. She said, “Dr. Yadaiah told that the vessels in the baby’s eyes were not developed accordingly and if regular eye check-up is not done it would gradually go into blindness.” The baby underwent laser treatment for ROP twice. Later on, before discharge of the baby, after screening for ROP the mother was told that the baby’s eyes were normal and there would be no problem.
The baby, of 1700 grams weight, was discharged from the hospital on April 29, 2016. As suggested by the hospital, the mother was ready to take the baby to hospital for monthly follow-up check-ups.
Dr Srinivas Murki, Newborn Care Mentor with baby Rishita
Rishita benefits from the use of a Sound Spa
Dr Subhadra Jalali, Eye Care Mentor, looks after baby Rishita
Tiny Rishita holds the finger of Dr Yadaiah, paediatrician in Nalgonda DH- Twins - Against All Odds
One of twin preterm babies of Sneha Kalokhe was referred from the district hospital (DH) in Nanded, a town over 400 km from Pune to it’s DH Neonatal Intensive Care Unit (NICU) for severe ROP. The preterm baby was treated successfully by the team from H V Desai Eye Hospital on 10th June 2017.
Sneha’s husband Bhimrao Kalokhe is a 28 year old young gentleman residing in remote village near Nanded district. He comes from poor socioeconomic background and works as a farm labrourer. He studied upto high school and then dropped out owing to family’s financial difficulties. His family of five (old parents, wife and a 5 year old daughter) are dependent on his meager daily earning of Rs. 300 (approximately 4.6 USD) per day. There are some days when there would be no farming which would be no work for Bhimrao.
Despite their poverty, the parents’ joy knew no bounds when they came to know of the twin pregnancy. Sneha, the mother went for regular antenatal care visits during the pregnancy but delivered prematurely at 33 weeks. She delivered in a private hospital and both the babies fell sick right after birth.
The twins weighed 1600 and 1700 grams respectively and doctors informed the parents that babies would require, oxygen and ventilation. They were admitted in the Neonatal Intensive Care Unit of the same hospital but the bill went up to Rs 56000 (USD 875) within a week. The family simply didn’t have money to pay the hospital or have any assets to sell. Thankfully their extended family came to their rescue and helped them pay the hospital bill. The parents were then forced to shift the twins to a government hospital where they could get free care.
Bhimrao was by the side of his wife for few days but could not afford to lose his income hence he had to leave his wife alone while the babies were being taken care in the SNCU. During that period the family was so short of money that sometimes they had to starve for a day or two. To add to their difficulties, Sneha got acute gastroenteritis during that period and had to be hospitalized adding to their financial burden.
Dr Chavan (paediatrician) from Nanded DH referred them to Dr Ghonsikar (ophthalmologist) for ROP screening. Dr Ghonsikar, a private practitioner who screens for ROP at Nanded DH noticed that one of the twins had severe ROP. Entire world came crashing down for the husband and wife when the ophthalmologist told them that both babies had ROP and could go blind if not treated on time. Both Sneha and her mother started crying. After so much of physical and emotional stress, they had to face another harsh reality.
The DH in Nanded did not have the facility to treat ROP in pre-term infants and the treatment was available only in few private hospitals. The parents could not afford to pay for the treatment in private hospitals and were advised to travel to Pune for the treatment. As laser treatment is expensive in private hospitals, Dr Ghonsikar referred them to DH Pune where free treatment could be availed. They chose to travel by train, a seven hour long journey with the newborn babies.
Dr Ashwini Sonawne, ophthalmologist from H V Desai Eye Hospital, went to Pune DH and performed laser on one of the twins who had severe ROP. When Dr Ashwini explained to them about need for follow up, parents readily agreed to stay in Pune for a week. During this stay, parents had to stay and sleep on the road as they could not afford to pay for a place to stay. Three adults had to share a meal of 2 Rotis (Indian bread) twice a day which Sneha was entitled to. They had no money to buy food.
Despite these hardships, they showed their utmost commitment for the welfare of their children and came back to H V Desai Hospital for follow up after a week. Dr Devika (neonatologist at Pune DH) and Dr Sirsikar (ophthalmologist) were kind enough to arrange free transport for follow up visit.
Parents were delighted to know that their baby’s ROP had started regressing and agreed to keep regular follow up with local ophthalmologist after going back to Nanded. They would also come back to Pune for follow up if advised by local ophthalmologist.
Coming to Pune proved a blessing in disguise for the family. Here they received all the support and counselling and free laser treatment for their child. Before leaving they thanked the H V Desai team and Pune DH for saving their daughter from going blind permanently.
* Name has been changed
Sneha Kalokhe with her twin babies, mother and husband at HV Desai Hospital, Pune, India
Laser in progress for Sneha’s baby at HV Desai Hospital, Pune, India





