


Policy Brief
Diabetic Retinopathy – a growing threat to sight in India
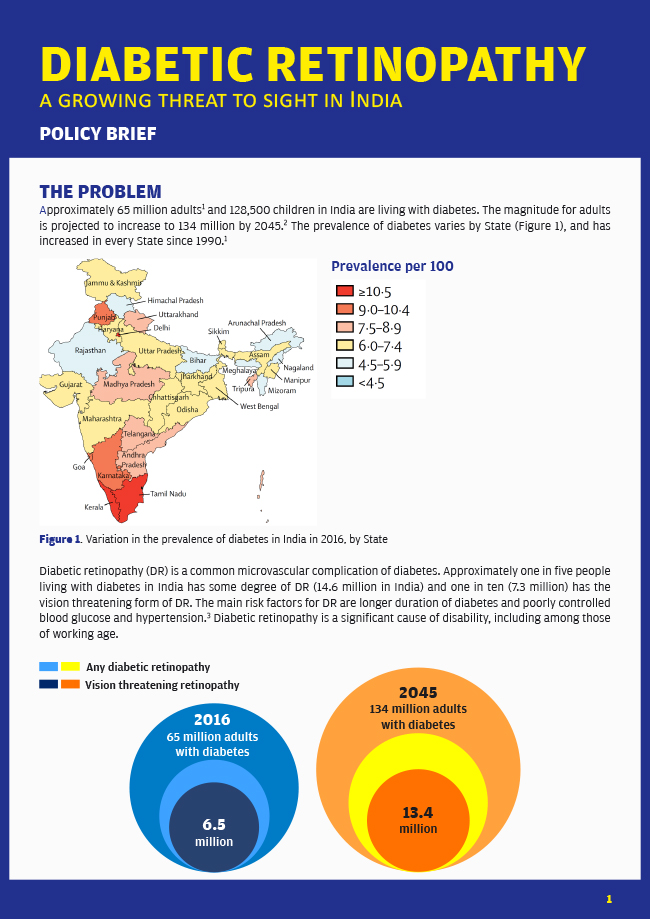
THE PROBLEM

- India State-Level Disease Burden Initiative Diabetes Collaborators. The increasing burden of diabetes and variations among the states of India: the Global Burden of Disease Study 1990-2016. Lancet Glob Health. 2018 Sep 11. pii: S2214-109X(18)30387-5. doi: 10.1016/S2214-109X(18)30387-5.
- International Diabetes Federation. India country report. Diabetes Atlas Eighth edition 2017. http://diabetesatlas.org/resources/2017-atlas.html
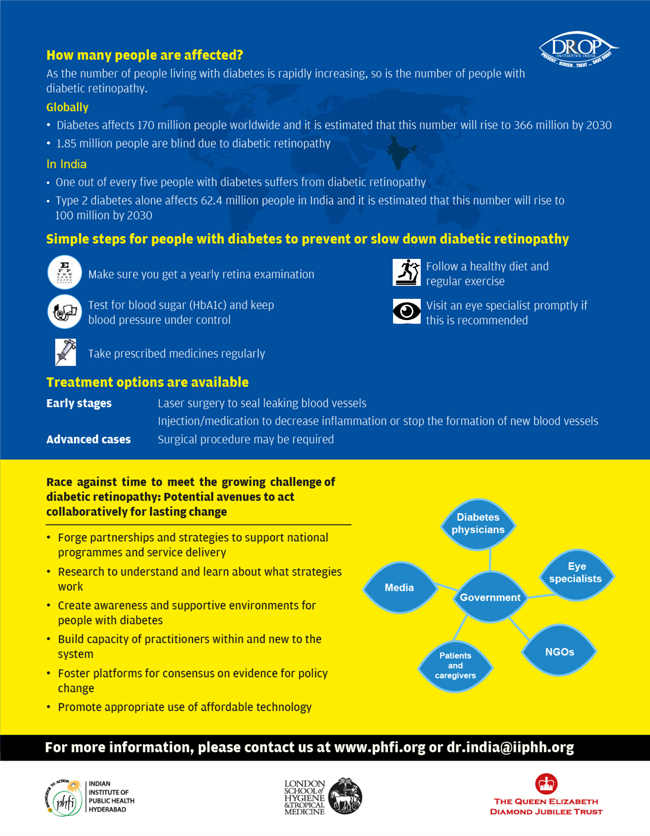
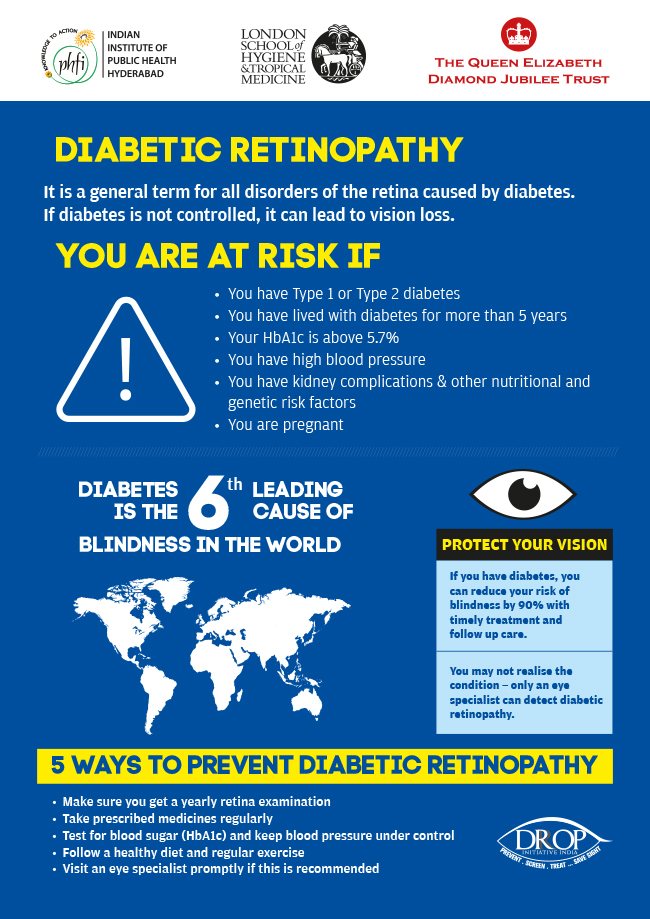
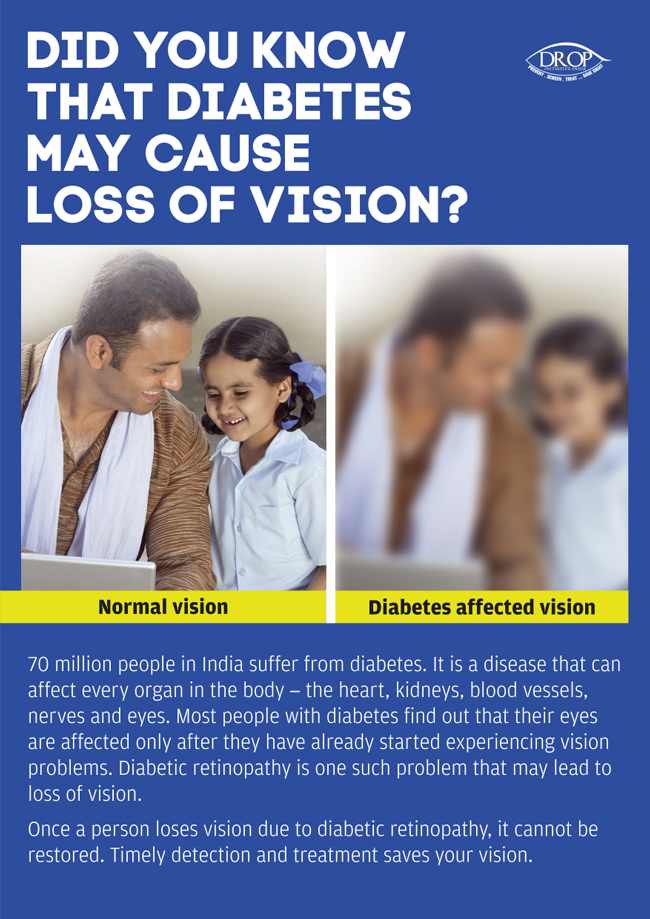
Diabetic Retinopathy (DR) is a common microvascular complication of diabetes.
The main risk factors for DR are longer duration of diabetes and poorly controlled blood glucose and hypertension. Diabetic Retinopathy is a significant cause of disability, including among those of working age.
The main risk factors for DR are longer duration of diabetes and poorly controlled blood glucose and hypertension. Diabetic Retinopathy is a significant cause of disability, including among those of working age.

Diabetic Retinopathy
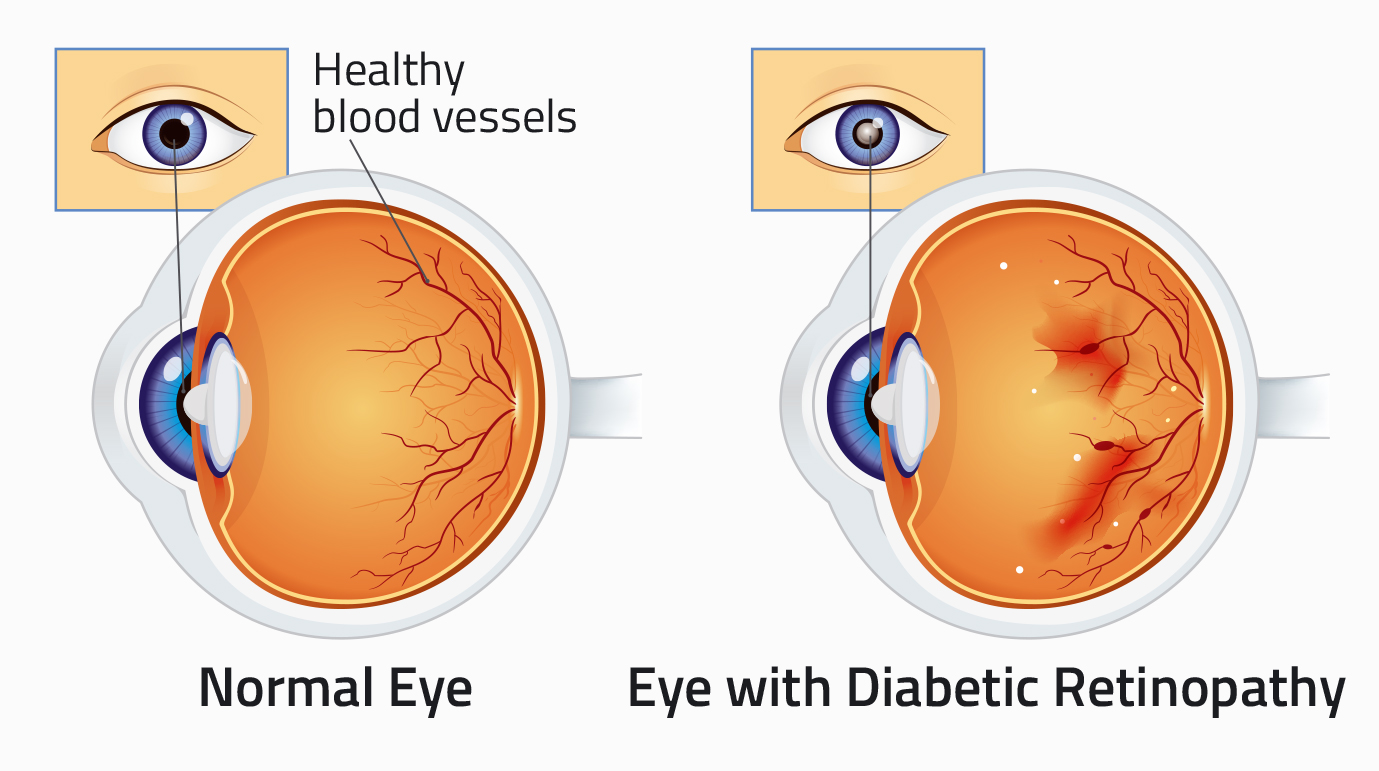
Diabetic Retinopathy results from damaged blood vessels in the retina, the light sensitive tissue which lines the inside of the back of the eye. The following mechanisms are implicated:
- Leaky blood vessels can cause swelling of the retina
- Blocked blood vessels cause damage because not enough oxygen reaches the retina
- Abnormal blood vessels can grow on the retina. These blood vessels can cause bleeding inside the eye
Once vision has been lost from DR, it usually cannot be restored.
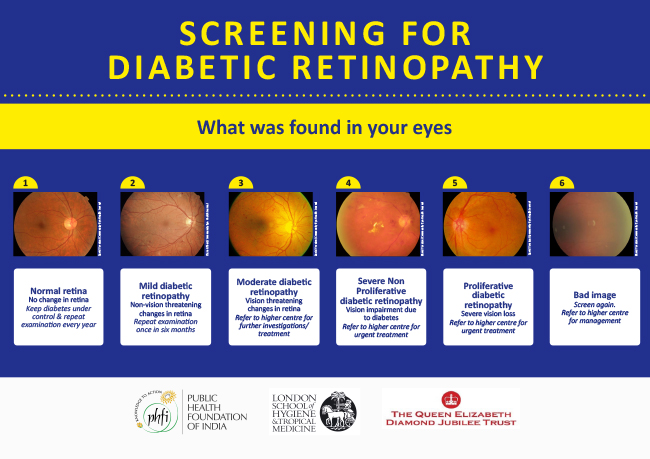
There is an international classification for DR, and the natural history is known. Some signs of DR are classified as mild, but others are classified as vision-threatening.
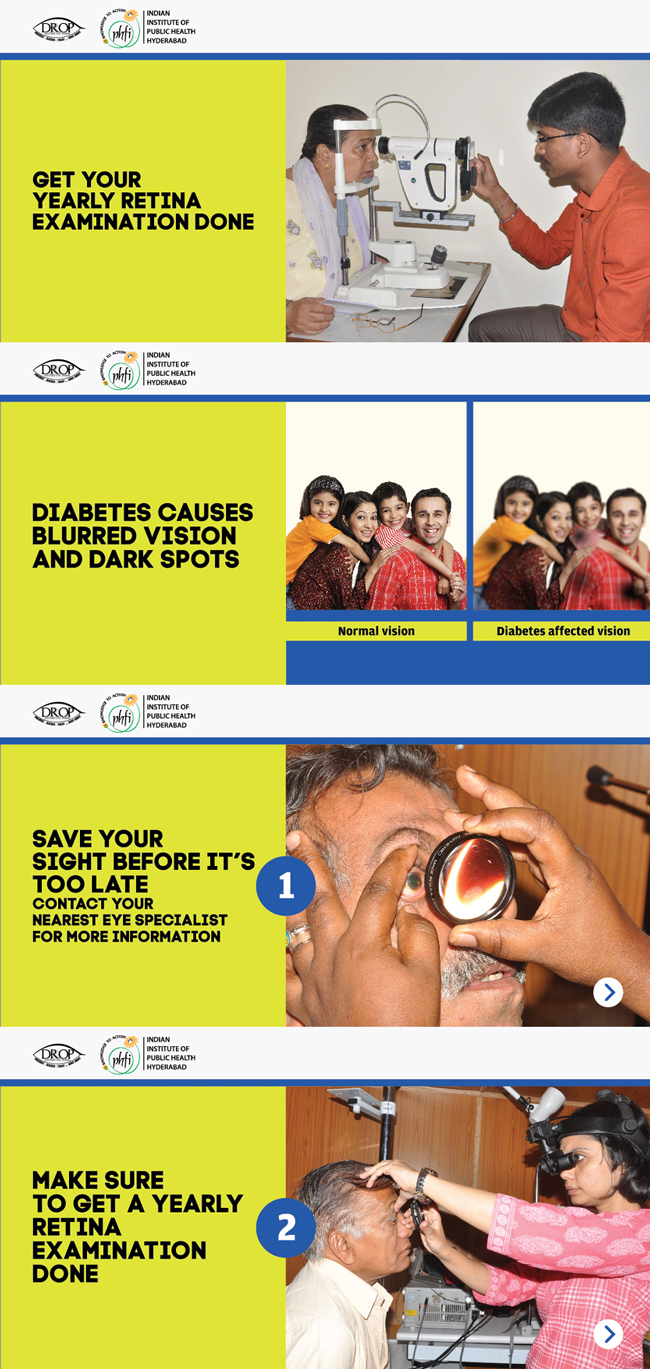
Vision testing or a torch light examination of the front of the eye cannot be used to assess whether DR is present, as even very severe DR does not always affect the vision, and the front of the eyes appear normal.
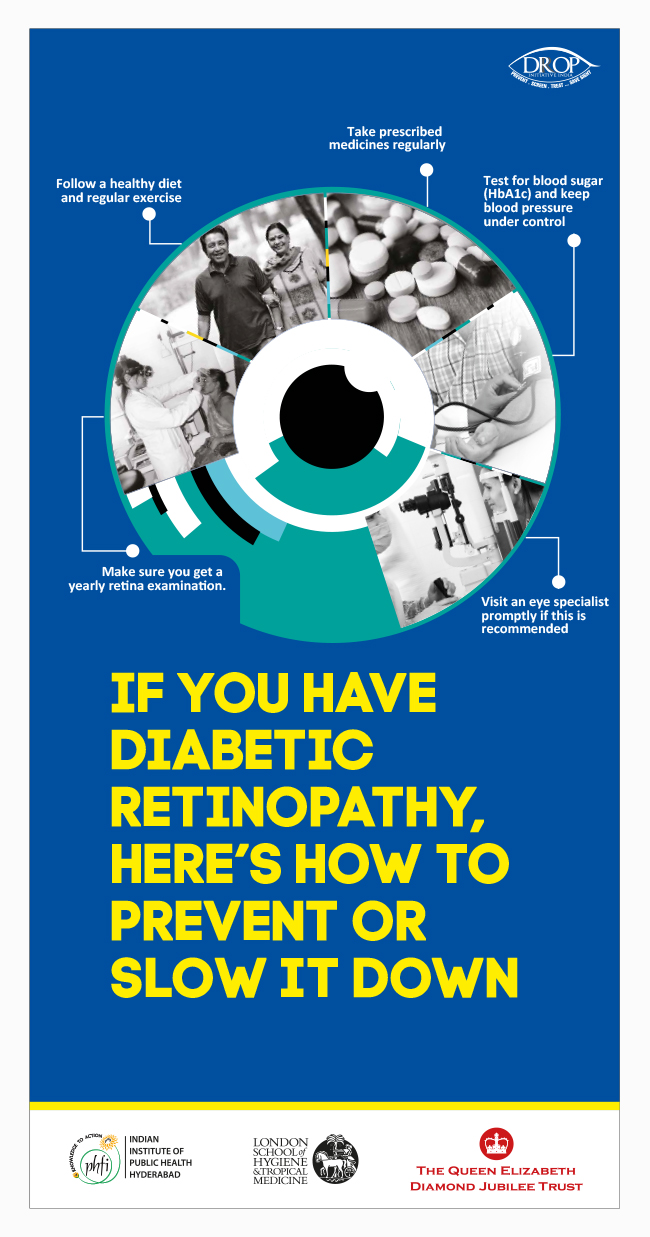
There is extensive evidence that good control of blood sugar and blood pressure reduce the risk of vision-threatening DR. This requires lifestyle changes, regular monitoring, and adherence to prescribed medication.
Strategies to reduce DR will also help reduce chronic kidney failure, cardiovascular disease and the other complications of diabetes.
 The purpose of screening is to detect DR requiring treatment before the patient presents with vision loss. Screening for DR entails detailed examination of the retina. The preferred method is digital retinal imaging. Low-cost imaging systems are available, and allied health professionals can be trained to reliably capture, store, and make a decision about whether DR is present or not, with quality assurance mechanisms provided by a specialist ophthalmologist. People with any DR need to be referred to the next level of health care for diagnosis, and treatment if required.
The purpose of screening is to detect DR requiring treatment before the patient presents with vision loss. Screening for DR entails detailed examination of the retina. The preferred method is digital retinal imaging. Low-cost imaging systems are available, and allied health professionals can be trained to reliably capture, store, and make a decision about whether DR is present or not, with quality assurance mechanisms provided by a specialist ophthalmologist. People with any DR need to be referred to the next level of health care for diagnosis, and treatment if required.
Screening should start at the time of diagnosis for adult-onset diabetes; screening should start at the onset of adolescence in children with diabetes. Annual screening is recommended for all.
After referral, further diagnostic tests are required to identify those needing treatment. One form of DR is treated by intraocular injection of agents such as Anti-VEGF drugs, which may need to be repeated. New blood vessels need to be treated by laser. More advanced disease requires complex surgery. All patients who have been treated for DR also require long-term follow up.
There is good evidence that early detection and timely treatment preserve vision.

Healthcare expenditure in India on diabetes was 8,713 million USD in 2017, but information on the costs of providing care for DR are limited: costs to the German health insurance scheme was 2.23 billion euros in 2002. A study in India showed that teleophthalmology screening for DR was cost-effective ($1320 per QALY) using World Health Organization thresholds.
Strategies to be embedded within Ayushman Bharat as part of comprehensive diabetes care, which should include other complications.
![]()
Community health workers
- Good record keeping of people with diabetes
- Behaviour-change communication about the complications of diabetes, including sight loss from Diabetic Retinopathy and the need for annual retinal examination (screening) for DR
![]()
Primary level NCD Clinics in PHCs and CHCs
- Improve registers of people with diabetes to identify and track access to those needing screening for DR
- Ensure medication (for diabetes and hypertension) is provided for three months, or even six months, for those with stable diabetes and hypertension, to reduce overcrowding and improve care in secondary level clinics
- Ensure provision of regular screening for DR within NCD clinics, and referral to district hospitals of those with DR
- Behaviour-change communication
![]()
Secondary level (District Hospitals)
- Ensure medication (for diabetes and hypertension) and insulin are provided for three months, or even six months for those with stable diabetes, to reduce overcrowding and improve care in NCD clinics
- Improve the quality of medical care; e.g. HbA1c testing and regular blood pressure monitoring
- Ensure regular screening for DR within NCD clinics
- Build the capacity of eye care providers in the diagnosis and management of vision-threatening DR, with referral of those needing more advanced care
- Ensure availability of Anti-Vascular Endothelial Growth Factor (VEGF) agents where a trained ophthalmologist is available
- Ensure Health Management Information Systems (HMIS) are in place to track uptake of referrals from primary care
- Behaviour-change communication
![]()
Tertiary level hospitals (Medical Colleges)
- Build the capacity of eye care providers in the diagnosis and management of complex DR
- Ensure availability of Anti-VEGF agents
- Provision of low vision and rehabilitation services for those with irreversible loss of vision
- Ensure HMIS systems are in place to track uptake of referrals from secondary care
Roles and responsibilities at all levels need to be clearly defined and standardized.
Providing services that are accessible and equitable for DR will impact on all aspects of the health system, including:
- financing
- governance (e.g., National Guidelines for DR)
- capacity building of training institutions and staff at each level of the health system, with task sharing
- providing infrastructure (e.g., dedicated space for screening in NCD clinics) and equipment for screening, diagnosis and treatment
- HMIS to track access, uptake of referrals and the outcome of treatment
Close collaboration and coordination between physicians and eye care providers is also critical, and synergies are needed between National Programme for Control of Blindness (NPCB) and National Programme for Prevention and Control of Cancer, Diabetes, CVD and Stroke (NPCDCS).
Providing equipment for diagnosing and treating DR will strengthen the health system as the same equipment can be used for many other retinal conditions, including Age-Related Macular Degeneration, which will increase in importance as the Indian population ages.
New, low-cost imaging systems, telemedicine, almost-real-time automated image analysis, and new-generation treatment offer hope for the future in the detection and management of DR.
![]()
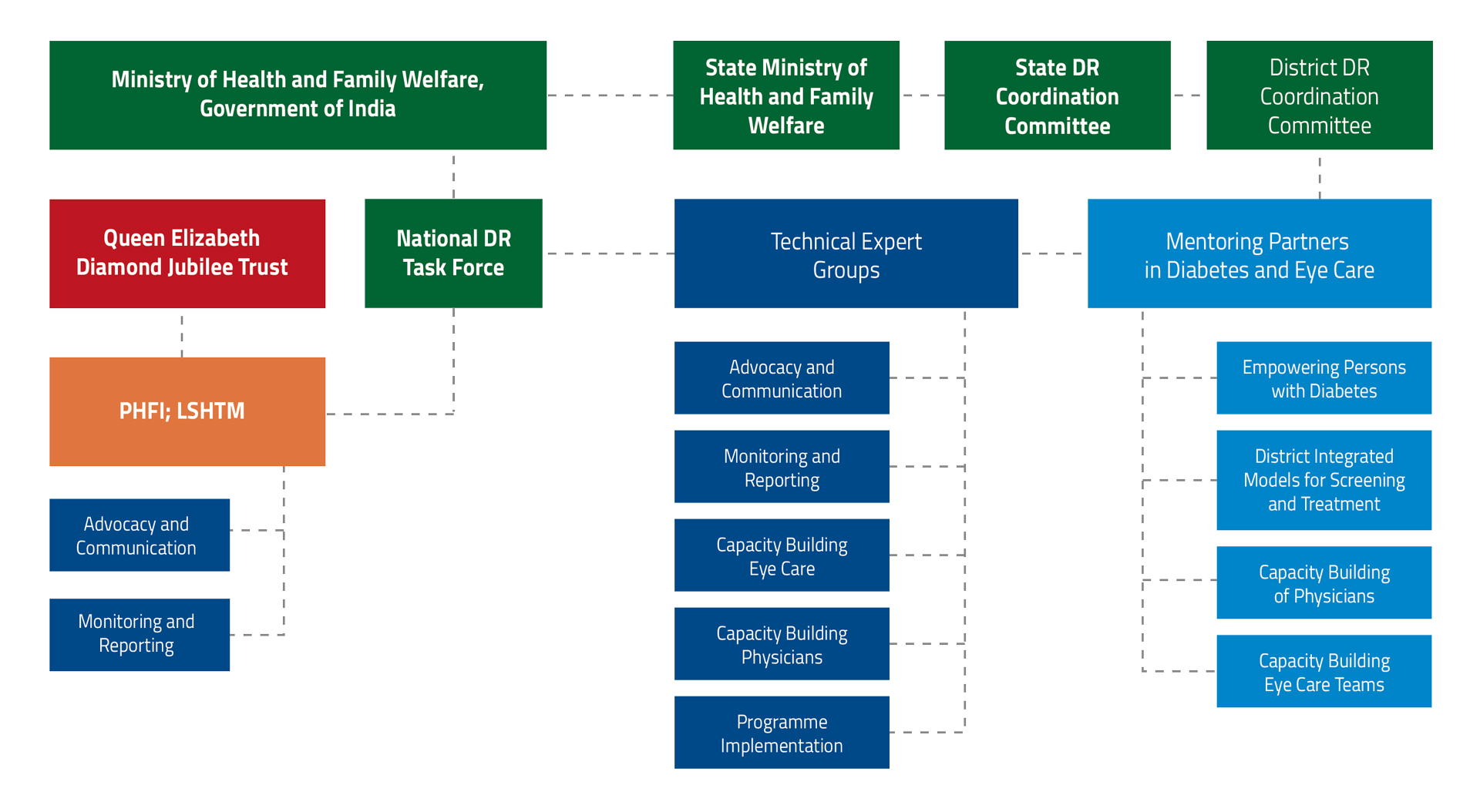
Terms of Reference for the National Task Force
The DR Taskforce will provide evidence-based advice to the government and health providers – both public and private – on DR prevention, control and management programmes and support the development of a national model DR-prevention strategy which is sustainable, accessible, scalable and integrated in the National Health Mission. The strategy will provide a blueprint for tackling the burden of preventable blindness currently caused by diabetes. It will be directed at the overall health sector in the model districts with a special focus on strengthening community awareness, screening and management at primary and secondary levels of health care.
Specifically, the Taskforce will:
- Support further development of the evidence base on DR, to inform the model DR strategy
- Provide advice for policy makers on the best ways for government investment in DR prevention
- Provide advice on the most effective strategies for targeting prevention in high-risk and underserved population groups
- Provide guidance to strengthen DR screening and management services, particularly in primary and secondary care settings
- Provide advice to government on options for better integration of DR services into the NHM
- Support the development of inter-departmental and multi-sectorial partnerships on DR
The Taskforce will report to the Ministry of Health and Family Welfare (MoHFW), Govt. of India.
The Taskforce will use a multidisciplinary approach, operate in a collaborative, open and consultative manner, and work in partnership with existing agencies and bodies working in associated departments.
The Taskforce will provide:
- Advice on the framework for the DR prevention project partnership between the Trust, PHFI, Minsitry of Health and Family Welfare (MoHFW) and the states
- Guidance to prepare a five-year work programme on DR
- Steering of the operations in the model districts through the district health societies
- Oversight and technical advice for project operations
- Advice on such matters as may be referred to the Taskforce from time to time by the MoHFW
- Inputs for a long-term DR prevention strategy for the country
The Taskforce shall be supported in its operations by a Secretariat based at the Public Health Foundation of India, New Delhi.
There will be no financial implication on the MoHFW for convening the meetings of the Task Force.
- Accountability and Deliverables
The Taskforce will report to the Ministry of Health and Family Welfare (MoHFW), Govt. of India.
The Taskforce will use a multidisciplinary approach, operate in a collaborative, open and consultative manner, and work in partnership with existing agencies and bodies working in associated departments.
The Taskforce will provide:
- Advice on the framework for the DR prevention project partnership between the Trust, PHFI, Minsitry of Health and Family Welfare (MoHFW) and the states
- Guidance to prepare a five-year work programme on DR
- Steering of the operations in the model districts through the district health societies
- Oversight and technical advice for project operations
- Advice on such matters as may be referred to the Taskforce from time to time by the MoHFW
- Inputs for a long-term DR prevention strategy for the country
The Taskforce shall be supported in its operations by a Secretariat based at the Public Health Foundation of India, New Delhi.
There will be no financial implication on the MoHFW for convening the meetings of the Task Force.
Terms of Reference for Technical Experts Group on Advocacy & Communication for Prevention of Sight-Threatening DR
- Assess and review existing government policies, government orders/directive orders and identify gaps for advocacy
- Review draft advocacy plan developed by PHFI for the Trust and amend as necessary
- Develop an advocacy strategy to support national programmes including an implementation plan
- Suggest advocacy materials and provide inputs for advocacy including identifying appropriate stake holders
- Develop a communication strategy and plan for the national programmes on NCD and blindness control
- Help in developing a resource kit for communication activities
- Periodically assess the progress towards identified activities and stated timelines
- Meet periodically to develop the strategy and to monitor progress
List of Members
| NAME | DESIGNATION | ORGANIZATION |
|---|---|---|
| Dr. GVS Murthy | Director, Indian Institute of Public Health, Hyderabad | Indian Institute of Public Health, Hyderabad, India |
| Dr. Raghupathy Anchala | Associate Professor, Indian Institute of Public Health, Hyderabad | Indian Institute of Public Health, Hyderabad, India |
| Dr. Clare Gilbert | Professor, Co-Director, International Centre for Eye Health, | London School of Hygiene & Tropical Medicine, London, United Kingdom |
| Dr. Usha Raman | Head of Department, Department of Communication | University of Hyderabad, Hyderabad, India |
| Sridivya Mukpalkar | Programme Associate, DR-ROP Team | Indian Institute of Public Health, Hyderabad, India |
| Gina Sharma | Senior Manager – External Communications & Digital Media | Public Health Foundation of India, New Delhi, India |
| Dr. Subhadra Menon | Director, Health Communication | Public Health Foundation of India, New Delhi, India |
| Dr. MK Garg | Endocrinologist | Army Hospital, New Delhi, India |
| Dinesh C Sharma | Science Editor | Mail Today, New Delhi, India |
| Dr. P V Rao | Endocrinologist | Nizams Institute of Medical Sciences, Hyderabad, India |
| Viswanath Kalluri | Chairman & Medical Director | Pushpagiri Vitreo Retina Institute, Hyderabad, India |
| Dr. Krishna Rao | Retina Specialist | Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India |
| Kavita Chauhan | Health Promotion Specialist | Public Health Foundation of India, New Delhi, India |
| MSS Gopal | Principal Correspondent | The Hindu, Hyderabad, India |
Terms of reference for Technical Experts Group on developing national guidelines for the prevention of sight-threatening DR, and for detection/screening and management of DR
- Review existing evidence for prevention, detection/screening and management of sight-threatening DR
- Review existing guidelines from other countries and adapt to Indian needs for prevention, detection/screening and management of DR
- Develop guidelines for implementation of screening and management programs for DR
- Periodically assess the progress towards identified activities and stated timelines
- Meet periodically to develop the strategy and to monitor progress
List of Members
| Name | Designation | Organisation |
|---|---|---|
| Nikhil Tandon | Professor & Head of Department | All India Institute of Medical Sciences, New Delhi, India |
| Dr. Damodar Bachani | Deputy Commissioner, Non-Communicable Diseases | Minsitry of Health & Family Welfare, New Delhi, India |
| Dr. Asim Sil | Medical Director | Vivekananda Mission Asram Netra Niramay Niketan, West Bengal, India |
| Clare Gilbert | Professor, Co-Director, International Centre for Eye Health, | London School of Hygiene & Tropical Medicine, London, United Kingdom |
| Dr. Purnima | Reaserch Assistant | Indian Institute of Public Health, Hyderabad, India |
| Dr. Praveen Vashist | Additional Professor | All India Institute of Medical Sciences, New Delhi, India |
| CS Yajnik | Diabetologist | King Edward Memorial Hospital, Pune, India |
| Viswanath Kalluri | Chairman & Medical Director | Pushpagiri Vitreo Retina Institute, Hyderabad, India |
| Kim Ramaswamy | Director Information Technology & Chief Medical Officer | Aravind Eye Hospital, Tamil Nadu |
| Dr. Pradeep Venkatesh | Professor | Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India |
Terms of reference for Technical Experts Group on capacity building of physicians and their teams for prevention of sight-threatening DR
- Improving capacity of physicians and their teams to control diabetes to reduce the complications of diabetes, including sight-threatening DR
- Improve physicians and their teams’ capacities for the detection of sight-threatening DR
- Develop learning objectives, curricula and evaluation matrix for the skill-up gradation programmes
- Advice on modalities for capacity building of support staff i.e. counselors/dieticians etc. to reduce the complications of diabetes including retinopathy
- Periodically assess the progress towards identified activities and stated timelines
- Meet periodically to develop the strategy and to monitor progress
List of Members
| Name | Designation | Organisation |
|---|---|---|
| Dr. Anura Kurpad | Founding Dean | St John’s Research Institute, Bengaluru, India |
| Dr. Nikhil Tandon | Professor & Head of Department | All India Institute of Medical Sciences, New Delhi, India |
| Dr. Nihal Thomas | Professor & Head, Department of Endocrinology | Christian Medical College, Vellore |
| Dr. Mohan | President & Founder | Madras Diabetes Research Foundation, Chennai, India |
| Sandeep Bhalla | Programme Director, Training | Public Health Foundation of India, New Delhi, India |
| Dr. Bipin Kumar Sethi | Endocrinologist | Care Hospitals, Hyderbad, India |
| Dr. Viswanath Kalluri | Chairman PVRI, Medical Director, Hyderabad | Pushpagiri Vitreo Retina Institute, Hyderabad, India |
| Dr. Yograj Sharma | Chief | Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India |
| Dr. Raghupathy Anchala | Associate Professor, IIPH Hyderabad | Indian Institute of Public Health, Hyderabad, India |
| Dr. Purnima | Reaserch Assistant | Indian Institute of Public Health, Hyderabad, India |
| D Prabhakaran | Vice President | Public Health Foundation of India, New Delhi, India |
| Dr. Brijendra | Diabetologist | Madras Diabetes Research Foundation, Chennai, India |
Terms of reference for Technical Experts Group on capacity building of ophthalmologists for management of Diabetic Retinopathy
- Assess specific needs for capacity building of ophthalmologists for managing Diabetic Retinopathy both in the short term (project period) and the long term (sustainable activities)
- Assess specific needs for capacity building of ophthalmology technician/optometrists in timely detection and referral of DR
- Develop learning objectives, competency-based curricula, and assessment methods
- Periodically assess the progress towards identified activities and stated timelines
- Meet periodically to develop the strategy and to monitor progress
List of Members
| Name | Designation | Organisation |
|---|---|---|
| Dr. Tara Prasad Das | Regional Chair | International Agency for the Prevention of Blindness |
| Dr. Rajalakshmi | Consultant Ophthalmologist | Madras Diabetes Research Foundation, Chennai, India |
| Dr. Rajiv Raman | Consultant | Sankara Netralaya, Chennai, India |
| Dr. Rajvardhan Azad | Principal Advisor | All India Institute of Medical Sciences, New Delhi, India |
| Dr. Narender Kumar | Deputy Director General | National Programme for Control of Blindness, New Delhi |
| Asim Sil | Medical Director | Vivekananda Mission Asram Netra Niramay Niketan, West Bengal, India |
| Dr. SC Shetty | Vice Chancellor | Sri Devaraj Urs Academy of Higher Education & Research |
| Dr. Quresh Maskati | President | All India Ophthalmological Society, New Delhi, India |
| Dr. Pradeep Venkatesh | Professor | Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute Of Medical Sciences, New Delhi, India |
| Dr. Dinesh Talwar | Senior Consultant | All India Institute of Medical Sciences, New Delhi, India |
Terms of reference for Technical Experts Group on data management for monitoring and evaluation: IT and HMIS
- To provide expert guidance on the data management tools required for M & E
- To review the developed HMIS framework for M & E
- Periodically review the progress of data collection the monitoring indicators developed in the HMIS framework
- Formulate ToR for mid-term and final evaluation
List of Members
| Name | Designation | Organisation |
|---|---|---|
| TulasiRaj RD | Executive Director Operations | Aravind Eye Hospital, Chennai |
| Dr. Renu Srivastava Goel | SNCU Coordinator | Minsitry of Health & Family Welfare, New Delhi, India |
| Dr. Anand Vinekar | Founder Secretary | Indian ROP Society |
| Rajiv Raman | Consultant | Sankara Netralaya, Chennai, India |
| Gagan Gupta | Health Specialist | UNICEF, India |
| Dr. Melissa Glenda Lewis | Senior Lecturer | Indian Institute of Public Health, Hyderabad, India |
| Ganesh | Senior Manager - Systems & IT | Aravind Eye Hospital, Coimbatore, India |
| Dr. Ajay Khera | Deputy Commissioner | Minsitry of Health & Family Welfare, New Delhi, India |
| PK Prabhakar | Deputy Commissioner | National Health Mission |
Terms of reference for Technical Experts Group on review of programme planning and implementation in Trust-supported districts
- Ratify operational guidelines developed for Trust-supported programmes
- Review proposals received from mentoring partners
- Support development of district-level models
- Provide technical input to mentoring partners
- Meet periodically to assess need for technical input
List of Members
| Name | Designation | Organisation |
|---|---|---|
| Dr. GVS Murthy | Director, Indian Institute of Public Health, Hyderabad | Indian Institute of Public Health, Hyderabad, India |
| Dr. Rajan Shukla | Associate Professor | Indian Institute of Public Health, Hyderabad, India |
| Dr. Clare Gilbert | Professor, Co-Director, International Centre for Eye Health, | London School of Hygiene & Tropical Medicine, London, United Kingdom |
| Dr. Krishna Murthy | Medical Director | Vittala International Institute of Ophtalmology |
| Nikhil Tandon | Professor & Head of Department | All India Institute of Medical Sciences, New Delhi, India |
| Prof. Yograj Sharma | Chief | Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India |
| Damodar Bachani | Deputy Commissioner, Non Communicable Diseases | Minsitry of Health & Family Welfare, New Delhi, India |
| Thulasiraj RD | Executive Director Operations | Aravind Eye Hospital, Chennai |
| Sara Varghese | Regional Director | Vision 2020 India |
| Kuldeep Dole | Deputy Medical Director | HV Desai Eye Hospital |
| Mohita Sharma | Chair Person & Founder | Tirupati Eye Centre |
| Dr. Rakesh Sahay | Professor & Head of Endocrinology | Osmania Medical College & Hospital |
| Narender Kumar | Deputy Director General | National Programme for Control of Blindness, New Delhi |
| Dr. Raghupathy Anchala | Research Associate, IIPH Hyderabad | Indian Institute of Public Health, Hyderabad, India |
| GV Rao | Executive Director | The HANS Foundation, Delhi, India |
| Dr. Mohan | President & Founder | Madras Diabetes Research Foundation, Chennai |
Terms of Reference for State/District Coordination Meetings
- State and district NCD and NPCB officers would act as nodal officers in charge for implementing the project in the state and would coordinate all the activities pertaining to the project
- There would be a coordination committee at the state and district level
- State level coordination committee will meet under the chairmanship of Secretary, Health at least twice a year.
- Members will be the Director Health Services, Director Medical Education, Director IIPH Hyderabad, and Nodal officer National Blindness Control programme, NPCDCS and representative of mentoring partners of states and others suggested by the Department of Health and Family Welfare, Government of respective states
- Review the project implementation
- District coordination committee will be established under the chairmanship of the district collector, respective project district
- The committee will meet every quarter with more frequent meetings in the first year, if necessary. Other members would be District Medical and health Officer, DPM, Deputy DMO in charge of NCD and Blindness Control Programme, PHFI Programme consultant in charge of the project and representative of mentoring partner and others suggested by Department of Health and Family Welfare, Government of respective state
- Review the progress of the project implementation activities
Governance Structure
Final TEG Outputs
1st TEG meeting on Advocacy and Communication Strategy, April 2015
- Terms of References for TEG on advocacy and communication were agreed upon in the first meeting
- Discussion on advocacy and communication strategies and the group came up with a major advocacy strategy, Tasks/Target audience, Communication activities, Materials
2nd TEG meeting on Advocacy and Communication Strategy, October 2015
ADVOCACY
- Establish linkages with other expert groups (TEG 2 – Guidelines, TEG-3/4 IT/HMIS) to know specific tasks/areas that need advocacy
- Emphasis on identification of systemic, behavioural, attitude, economic barriers for the advocacy and communication strategies and Use partner networks in the local advocacy and communication activities
- Data gaps: The group identified issues with gaps in understanding of the literature. The group suggested conducting a targeted/systematic review of Diabetic Retinopathy literature in India with best practices and strategies followed in other countries.
COMMUNICATIONS
- The group advised to ensure the quality of the educational materials that are to be developed. Campaigns and peer groups can be established in the program implementing states
- Conduct workshops in all eight districts regarding the communication strategies. Formation of self-care groups and propagation of information on radio, newspaper. Use of Social media effectively
3rd TEG meeting on Advocacy and Communication Strategy, February 2017
- The Technical expert group members were provided with developed Information Education Communication material on Diabetic retinopathy (posters, leaflet, videos etc) to review by Indian Institute of Public Health staff
- Group members were asked to identify the progressions that should be included in the given material so that they will have larger impact on people
1st TEG meeting on National Guidelines for Diabetic Retinopathy, November 2015
- National Guidelines for Diabetic Retinopathy can be developed in a phased manner, based by adaptating existing guidelines with evidence from India. The scope of the guidelines needs to be finalized, and a committee will define the scope of the guidelines
- Given the wide variation in health systems across India, the guidelines can be aspirational (i.e. would be in place given adequate resources) as well as practical (i.e. the minimum that needs to be in place)
- It is important that the recommendations are implementable, and information collected over the next few months from the Trust supported programme can be used to this end
- A Guideline Development Group and an External Review Group, with appropriate representation, will be convened to take the work forward
2nd TEG meeting on National Guidelines for Diabetic Retinopathy, March 2016
- Reviewed and amendment of PICO (Problem Intervention/Indicator Comparison Outcome) questions listed in the Australian Diabetic Retinopathy Guidelines
- Recommendations – minimum information to be collected as part of generic data collection for diabetics / Non Communicable Disease form
- Develop an online system for routine data collection and pilot test it in the Trust programme
- Modifications to be made in Vision 2020 DR guidelines
- Dr.Rohan Chariwala and Dr. Sishendu Mahato will volunteer to work with the guideline committee to draft the national guidelines
- Scoping committee to be constituted by the experts from the Certificate Course Diabetic Retinopathy course- ophthalmologists, physicians and public health experts
- Prof Clare Gilbert to contact Iris Gordon and Spenser Haddon to explore the opportunities for medical writing expert to draft the guidelines based on inputs from the experts
3rd TEG meeting on National Guidelines for Diabetic Retinopathy, March 2016
- Scoping Committee has prioritized and finalised a draft scope of guidelines
- Dr Rohan Chariwala to work along with Dr Clare. Iris Gordon to develop the search terms for the evidence-base
- Iris to draw up search terms (India; Singapore; Hong Kong; China; Bangladesh; Pakistan; Nepal; Sri Lanka; Thailand; Indonesia; Malaysia; Philippines; Middle East)
- Fixed timelines for the guidelines development – each section has been divided into further sub sections and the committee has assigned the topics to individuals
- Permission letters to be written to the Vision 2020 members seeking permission to update guidelines and also to seek permission of the Australian group and UK group to use/adapt material used in them
4th TEG meeting on National Guidelines for Diabetic Retinopathy, July 2016
- Draft guidelines presented at the 4th TEG meeting
- Recommendations for PICO (Problem Intervention/Indicator Comparison Outcome) questions
- Review of PICO (Problem Intervention/Indicator Comparison Outcome) from other countries reviewed
- Recommendation to convene a guidelines working group: Members of the group to include Dr.Rohan Chariwala, Prof. Clare Gilbert, Dr.Hayden Spencer, Dr. Asim Sil’s Dr. Shirshendu Mahato, Jenny Evans and 1 or 2 physicians
- By the end of August Working Group members to:
- Ensure remaining chapters are submitted – Rohan to follow up
- Tabulate PICOs (Indian) and recommendations from other countries – Hayden and Clare
- Finalise coding of studies from systematic review – Hayden, Iris, Clare
- Get full pdfs of papers from SLR, by PICO question – Iris and Clare
5th TEG meeting on National Guidelines for Diabetic Retinopathy, February 2017
- Suggestion to add a section on cataract and a section on vitrectomy
- Evidence should be used. Surgical (4.5) and non-Surgical (4.6) should be put under the same section
- Allocation of sections (that are pending)
- Section 8.5 to be written by Dr.Rajeev Raman
- Section 8.6 and 8.7 to be written by Dr. Thulasi Raj
- Section 8.8 Dr. Nikhil Tandon and Dr. Usha Raman
- Section 8.9 Dr. Bachani
- Recommend an interface between National Programme on Control of Blindness and Non Communicable Disease; build on same lines as diabetes and Tuberculosis
- Costing to be moved to economics chapter
- Section on competency to be a stand-alone chapter
- Identification of external reviewers to review the guidelines. Look at authors of other guidelines. Suggestion: Indian Retina specialists, Dr. Vineet and Dr. Geetha
- Suggestion to have a two-phase review
6th TEG meeting on National Guidelines for Diabetic Retinopathy, 24 May 2019
Endocrinologists – 24 May 2019
Ophthalmologists – 28 May 2019
- Review and finalization of the technical guidelines pertaining to the endocrinology portion and ophthalmology portion by respective experts by means of voting. (Proxy voters were employed to vote on behalf of experts who were unable to be present physically)
- Future plans were discussed and the following action points were realised:
- Publishing of Technical guidelines
- Revision of recommendations after 5 years to incorporate the new technological advancements and evidences by then
1st TEG meeting on Capacity Building of Physicians and their Teams for Prevention of Sight-Threatening DR, 4 March 2015
- Discussion on developing a Certificate Course for Evidence-Based Management of DR (CCEDDR) which is renamed as Certificate Course on Prevention of Blindness due to Diabetic Retinopathy (CCPBDR)
- Decision on Academic Partners to design eye care modules
- Aravind Eye Care
- Mohans Diabetic Research Institute
- All India Institute of Medical Sciences, Delhi including RP Centre
- Consideration of capacity building of allied health professionals like optometrists, dieticians for the opportunistic awareness creation on Diabetic Retinopathy
1st TEG meeting Capacity Building of Ophthalmologists, April 2015
- Terms of references for expert group on capacity building of ophthalmologists meetings agreed upon
- Modalities regarding capacity building of the ophthalmologists were discussed
2nd TEG meeting on Capacity Building of Ophthalmologists for Management of Diabetic Retinopathy, June 2015
- Plans and activities for developing medical retina course curriculum finalised
- Discussion on competency-based framework initiated
- Master trainers identified for the teaching capacity building for ophthalmologists
- Suggestions from the experts group members include:
- Letters to the training institutes need to be sent to know a) their willingness to train in medical retina for Diabetic Retinopathy using a standardized, competency based curriculum, which includes hands-on training, and b) number of candidates they can train a year under National Programme on Control of Blindness sponsorship.
- Develop a standard certified course for PMOA (Paramedic Ophthalmic Assistants) at vision centres in Primary Healthcare centres
3rd TEG meeting on Capacity Building of Ophthalmologists for Management of Diabetic Retinopathy, September 2015
- Contents of Diabetic Retinopathy manual were discussed
- Abdominal obesity and role of hypertension in Diabetic Retinopathy to be added in the manual
- Format for training, assessment and evaluation were discussed
- Certificate Course on Evidence-Based Diabetic Retinopathy to begin in regional training centers across India. Medical Officers from National Program on Control of Blindness and districts for training were recommended to be candidates for training
- A discussion on whether the manual should include a training for Para Medical Ophthalmic Assistants
1st TEG on Data Management for Monitoring and Evaluation, March 2015
- Terms of references for expert group on data management meetings agreed upon
- Changes suggested to monitoring and evaluation framework. Impact indicators for implementing districts were recommended
- Formats for the monitoring and evaluation framework are to be developed within agreed time lines
2nd TEG on Data Management for Monitoring and Evaluation: Information Technology and Health Management Information System, October 2015
- Data management tools for Diabetic Retinopathy project formulated
- Planning for midterm and final evaluation and criteria for the evaluation and selection of agency for the evaluation in progress
1st TEG meeting on Review Programme Planning and Implementation in Project Districts, July 2015
Medication must be given after screening for Diabetic Retinopathy and Diabetes Mellitus. One on one counselling for patients must be given when health care givers communicate diagnosis and available treatment options to the patients.
- Patients should have ½hr-1hr training where Diabetes Mellitus patients are taught about comprehensive Diabetes Mellitus care. It was also suggested by the group members that developing aa ‘Total diabetic care’ book, by the partners, could be very useful for the patients ( like a hand book consisting of personal details along with medical history) for them to understand the holistic care that is required for the management of diabetes
- Aadhaar number could be used as unique ID to track patients and the same can be made mandatory in all the databases of the implementing partners
Diabetic Retinopathy Android Application
 Diabetic Retinopathy Application on Android Tablet is designed to capture patient information, eye screening results, patient follow-ups, scheduled appointments and patient reports. It syncs this data with the web version of this application, so patient data is available on both the versions.
Diabetic Retinopathy Application on Android Tablet is designed to capture patient information, eye screening results, patient follow-ups, scheduled appointments and patient reports. It syncs this data with the web version of this application, so patient data is available on both the versions.
The Web and Android Tablet will stay in sync via the Internet. The server database that will store all the details entered in the Web application will also act as a repository for the data saved in the tablet version of the application.
In case the internet is not available or is unstable, the data from the tablet will be stored in its local database.
The complete user guide to the Diabetic Retinopathy app is available to download here.



Links to Training Institutions under the Project
| State | Training Institution | Website |
|---|---|---|
| Andhra Pradesh | PVRI Hyderabad | |
| Goa | HV Desai Eye Hospital, Pune (Current training institution for Ophthalmologists from Goa) | |
| Gujarat | Divyajyoti Trust, Mandvi, Surat (Dist.) | |
| Karnataka | VIIO Bangalore | |
| Kerala | Little Flower Hospital, Thrissur | |
| Maharashtra | MGIMS, Wardha | |
| Odisha | LV Prasad Eye Institute, Bhubaneshwar | |
| Rajasthan | Global Hospital, Mount Abu | |
| Tamil Nadu | Aravind Eye Hospital, Tirunelveli | |
| West Bengal | VMANN, Rural West Bengal | n/a |
Case Studies
Santhanaraj (43) is living with his family at Thisayanvilai town in Radhapuram Block. He is working in a small textile shop at Thisayanvilai for a meagre income. He has two children and his wife is a working for daily wage by rolling Beedis (Tobacco rolled in Peepal tree leaves for smoking, similar to cigarettes). He has diabetes for the past 8 years. Two years ago, he felt some change in his vision but he didn’t take any treatment. While he was visiting Thisayanvilai PHC to collect the diabetes drugs, he came to know about the project. He was screened by the NCD staff at PHC and diagnosed with Mild NPDR (SUPEROTEMPORAL BRVO) on his left eye (newly diagnosed as DR). He was referred to Aravind Eye Hospital, Tirunelveli. He underwent investigations at the hospital and was advised to take injection.
He was administered with an IVTA injection at free of cost through the project. After the treatment, he feels improvement in his vision. He has been advised to take one more injection but due to his personal commitments, he didn’t visit the hospital on time. He feels happy about the project and the services rendered by the project at free of cost. He has to live with diabetes for long years and this project is an eye opener for him to know about the impact of diabetes on eye sight.

A.Ganesan (44) is living with his wife at Marunthampudhur village in Pappakudi Block. He and his wife both are HIV+ patients. The couple has no children.
He has DM for the past 8 years. He has been taking treatment at PHC, Maruthanputhur for Diabetes. Ganesan is working in a small hotel in his village for daily wages. He is the only bread winner of his family. He is regularly visiting the PHC at Maruthampudhur for routine health check-up and to get medicines for diabetes. He had done preliminary screening for Diabetic Retinopathy at the PHC thorough the Project and was diagnosed with MILD NPDR on both eyes and was advised to go for further examination by the retina doctor at Aravind Eye Hospital, Tirunelveli.
The doctor at Aravind Eye Hospital had done detailed examination and advised him to go for PRP LASER Treatment on both his eyes. He took free LASER treatment on 09.05.17 & 12.05.17. After the laser treatment he feels some improvement in his vision. The counsellor had explained him about the importance of maintaining the sugar level and the periodical eye check-up as prescribed by the doctors.
He thanked the Project, Aravind Eye Hospital and the PHCs for their remarkable service rendered at his village and helped him to save his vision to survive in the world. He added that this project is very useful to poor people like him.

“Only on that day of screening, I came to know that every diabetic patient should check their eyes every year for DR.”
Mrs.Mary (67) hails from a middle class family living with her husband at Thisayanvilai. Her husband is running a petty shop and the family survives with the income from it. She has two children and both of them have got married and living in different places.
10 years ago, Mrs. Mary got diagnosed with Diabetes in a private hospital. She took treatment for some years and then she stopped taking medication. Five years back she visited Thisayanvilai PHC and start continuing her treatment for diabetes. While she was doing her Cataract Surgery, she was diagnosed with DR, but she could not continue the treatment due to her financial constraints.
During December 2016, while she visited Thisayanvilai PHC, the NCD Nurse advised her to screen for Diabetic Retinopathy. The preliminary screening shown that, she had DR ( BE- Moderate NPDR). She was referred to Aravind Eye Hospital for further investigation. She visited AEH-TVL on 13.03.2017 and diagnosed with DR RE-Mod NPDR and LE- Severe NPDR with CSME. Doctors advised her to go for OCT investigation. She was administered with Avastin injection in her LE on 25.03.2017 & 04.04.2017 and in her RE on 13.05.17 at free of cost. After the treatment she has better vision. Due to her family commitment she could not come regularly for the follow-up at AEH-TVL. She has been consciously given counselling to continue her treatment.
She is so grateful to the QEDJT-DR Project, through which she could receive treatment for DR at free of cost. She wants this service to continue in all PHCs so that diabetic patient like her will be benefited. She also wishes to have treatment facility for DR in all PHCs so that poor people will be benefited and they need not travel to Tirunelveli to avail the treatment.

“Treatment facility for DR should be available in PHC so that poor people will be benefited and they need not travel to Tirunelveli to avail treatment.”
Mrs.Thangammal (61) is a widow and a resident of Poochikadu a small village near Thisayanvilai. She lost her husband 25 years ago. She has 5 children and all of them are got married and living in different places. She toiled a lot in the past to earn money to settle her children. Now she is surviving with her own earnings. She makes palm fibre baskets and furnishings and drapes using garment wastes.
She had diagnosed with Diabetes 6 years ago and has been taking treatment at Thisayanvilai PHC. She had blurred vision for a long time. Due to her financial condition and no one to accompany her to hospital, she simply ignored her eye problem.
On 23.02.2017, while she came to Thisayanvilai PHC to collect Diabetes medicine, the NCD nurse suggested her to do DR screening. While she was screened with the help of fundus camera, the preliminary screening revealed that she had DR on both eyes. She was immediately referred to Aravind Eye Hospital, Tirunelveli for further investigation. She visited AEH-TVL on 07.04.2017 and was confirmed with Moderate NPDR with CSME in RE. The doctor advised for Focal Laser and she was administered with Focal Laser on 13.04.2017.After the treatment her vision in RE improved and her existing vision is retained.
She thanks the QEDJT-DR Project for its wonderful service to poor. Since her eye sight is important for her survival, she realises the importance of the project through which poor people like her is benefited.

“Since my eyesight is important for my survival, I realise the importance of the project through which poor people like me are benefited.”
- Santhanaraj
Santhanaraj (43) is living with his family at Thisayanvilai town in Radhapuram Block. He is working in a small textile shop at Thisayanvilai for a meagre income. He has two children and his wife is a working for daily wage by rolling Beedis (Tobacco rolled in Peepal tree leaves for smoking, similar to cigarettes). He has diabetes for the past 8 years. Two years ago, he felt some change in his vision but he didn’t take any treatment. While he was visiting Thisayanvilai PHC to collect the diabetes drugs, he came to know about the project. He was screened by the NCD staff at PHC and diagnosed with Mild NPDR (SUPEROTEMPORAL BRVO) on his left eye (newly diagnosed as DR). He was referred to Aravind Eye Hospital, Tirunelveli. He underwent investigations at the hospital and was advised to take injection.
He was administered with an IVTA injection at free of cost through the project. After the treatment, he feels improvement in his vision. He has been advised to take one more injection but due to his personal commitments, he didn’t visit the hospital on time. He feels happy about the project and the services rendered by the project at free of cost. He has to live with diabetes for long years and this project is an eye opener for him to know about the impact of diabetes on eye sight.
- A. Ganesan
A.Ganesan (44) is living with his wife at Marunthampudhur village in Pappakudi Block. He and his wife both are HIV+ patients. The couple has no children.
He has DM for the past 8 years. He has been taking treatment at PHC, Maruthanputhur for Diabetes. Ganesan is working in a small hotel in his village for daily wages. He is the only bread winner of his family. He is regularly visiting the PHC at Maruthampudhur for routine health check-up and to get medicines for diabetes. He had done preliminary screening for Diabetic Retinopathy at the PHC thorough the Project and was diagnosed with MILD NPDR on both eyes and was advised to go for further examination by the retina doctor at Aravind Eye Hospital, Tirunelveli.
The doctor at Aravind Eye Hospital had done detailed examination and advised him to go for PRP LASER Treatment on both his eyes. He took free LASER treatment on 09.05.17 & 12.05.17. After the laser treatment he feels some improvement in his vision. The counsellor had explained him about the importance of maintaining the sugar level and the periodical eye check-up as prescribed by the doctors.
He thanked the Project, Aravind Eye Hospital and the PHCs for their remarkable service rendered at his village and helped him to save his vision to survive in the world. He added that this project is very useful to poor people like him.
“Only on that day of screening, I came to know that every diabetic patient should check their eyes every year for DR.”- Mary
Mrs.Mary (67) hails from a middle class family living with her husband at Thisayanvilai. Her husband is running a petty shop and the family survives with the income from it. She has two children and both of them have got married and living in different places.
10 years ago, Mrs. Mary got diagnosed with Diabetes in a private hospital. She took treatment for some years and then she stopped taking medication. Five years back she visited Thisayanvilai PHC and start continuing her treatment for diabetes. While she was doing her Cataract Surgery, she was diagnosed with DR, but she could not continue the treatment due to her financial constraints.
During December 2016, while she visited Thisayanvilai PHC, the NCD Nurse advised her to screen for Diabetic Retinopathy. The preliminary screening shown that, she had DR ( BE- Moderate NPDR). She was referred to Aravind Eye Hospital for further investigation. She visited AEH-TVL on 13.03.2017 and diagnosed with DR RE-Mod NPDR and LE- Severe NPDR with CSME. Doctors advised her to go for OCT investigation. She was administered with Avastin injection in her LE on 25.03.2017 & 04.04.2017 and in her RE on 13.05.17 at free of cost. After the treatment she has better vision. Due to her family commitment she could not come regularly for the follow-up at AEH-TVL. She has been consciously given counselling to continue her treatment.
She is so grateful to the QEDJT-DR Project, through which she could receive treatment for DR at free of cost. She wants this service to continue in all PHCs so that diabetic patient like her will be benefited. She also wishes to have treatment facility for DR in all PHCs so that poor people will be benefited and they need not travel to Tirunelveli to avail the treatment.
“Treatment facility for DR should be available in PHC so that poor people will be benefited and they need not travel to Tirunelveli to avail treatment.”- Thangammal
Mrs.Thangammal (61) is a widow and a resident of Poochikadu a small village near Thisayanvilai. She lost her husband 25 years ago. She has 5 children and all of them are got married and living in different places. She toiled a lot in the past to earn money to settle her children. Now she is surviving with her own earnings. She makes palm fibre baskets and furnishings and drapes using garment wastes.
She had diagnosed with Diabetes 6 years ago and has been taking treatment at Thisayanvilai PHC. She had blurred vision for a long time. Due to her financial condition and no one to accompany her to hospital, she simply ignored her eye problem.
On 23.02.2017, while she came to Thisayanvilai PHC to collect Diabetes medicine, the NCD nurse suggested her to do DR screening. While she was screened with the help of fundus camera, the preliminary screening revealed that she had DR on both eyes. She was immediately referred to Aravind Eye Hospital, Tirunelveli for further investigation. She visited AEH-TVL on 07.04.2017 and was confirmed with Moderate NPDR with CSME in RE. The doctor advised for Focal Laser and she was administered with Focal Laser on 13.04.2017.After the treatment her vision in RE improved and her existing vision is retained.
She thanks the QEDJT-DR Project for its wonderful service to poor. Since her eye sight is important for her survival, she realises the importance of the project through which poor people like her is benefited.
“Since my eyesight is important for my survival, I realise the importance of the project through which poor people like me are benefited.”





